
The Tresiba® (insulin degludec) molecule is different by design
There are a number of reasons why once-daily Tresiba® may be the right option for your appropriate patients with diabetes starting on or switching to basal insulin, including a slow and steady release and a long duration of action.1-3
Flat and stable profile
Tresiba® (insulin degludec) injection 100 U/mL concentrations remained stable from day to day at steady state1-3
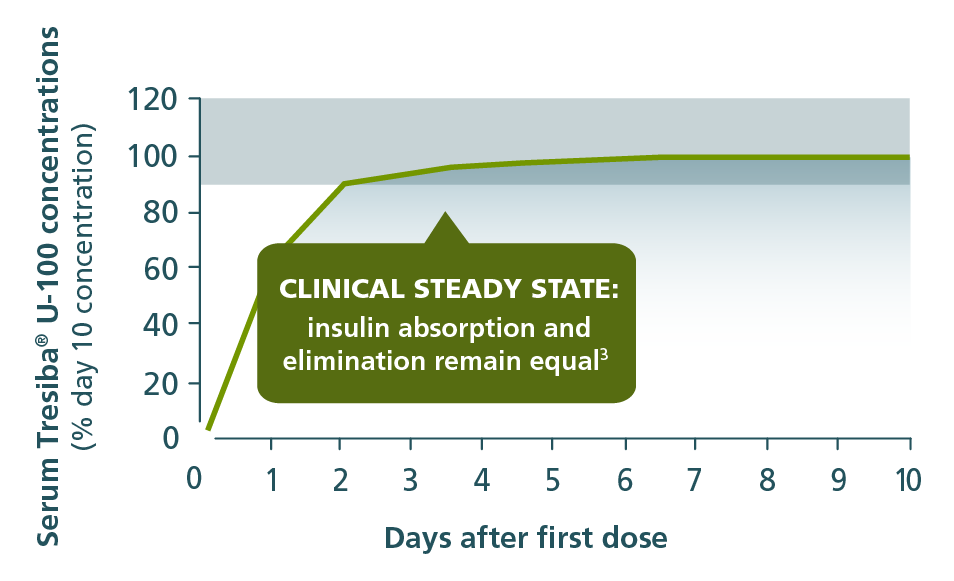
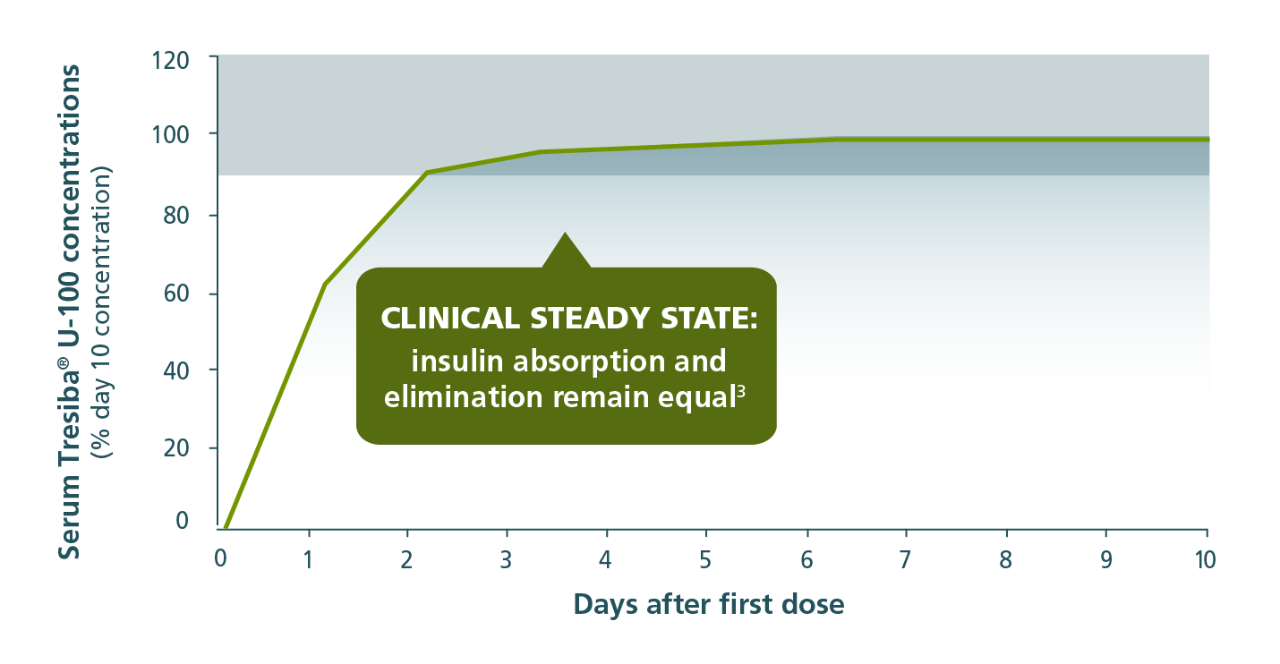
Values are estimated ratios relative to day 10; clinical steady state is defined as >90% of the final plateau level.2
- The recommended time between dose increases is 3 to 4 days (the same amount of time it takes to reach steady state)1

The Tresiba® half-life is approximately 2X longer than insulin glargine U-1002,4
42+ hour duration of action
Tresiba® U-100 is a basal insulin proven to last 42 hours—that won’t taper off at the end of the day1,5-7,a
A consistent routine is important, but if life gets in the way of a scheduled dose, Tresiba® provides continued efficacy.1
- Tresiba® was studied at alternating once-daily dosing intervals of 8 to 40 hours in adult patients1
- Adult patients who miss a dose of Tresiba® should inject their daily dose during waking hours upon discovering the missed dose, then continue with their regular dosing schedule1
- Adult patients should wait at least 8 hours between Tresiba® injections1
aAfter the last of 8 once-daily injections (0.4 units/kg).
A basal insulin that gives adult patients the option to change day-to-day dose timing if needed1
Less within-subject variability
Patients on Tresiba® U-100 experienced less within-subject day-to-day variability vs insulin glargine U-100
One dosing interval
Tresiba® U-100 had 4X less within-subject, day-to-day variability vs insulin glargine U-1003
Calculated using the glucose infusion rate (GIR) profiles of adults with type 1 diabetes (P<0.0001)
One dosing interval (0-24 h) at steady state
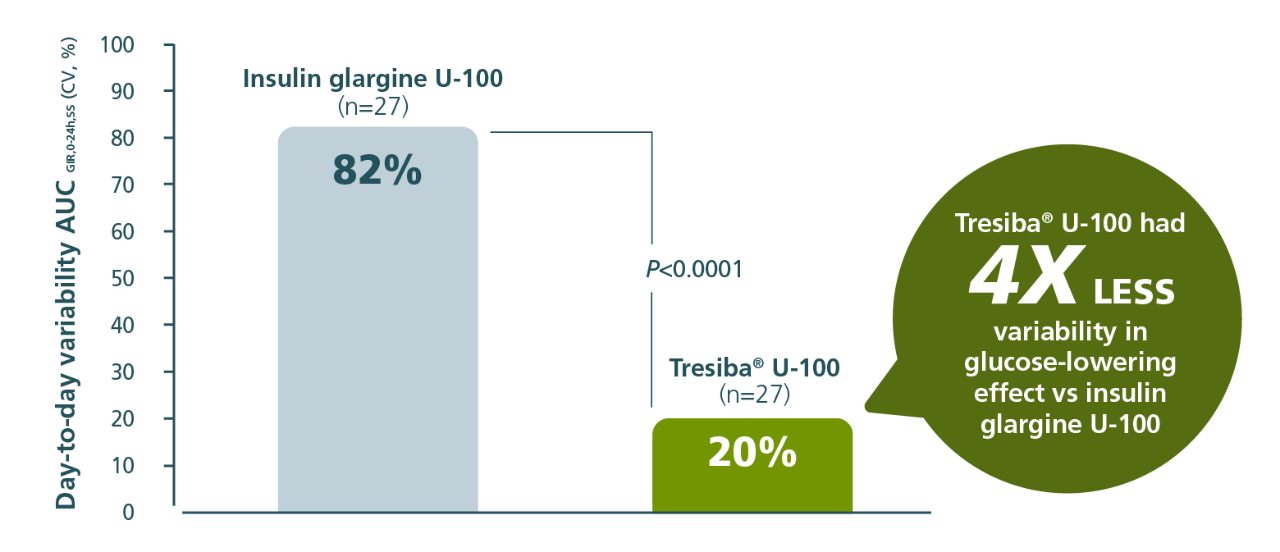
The clinical significance of these PK/PD differences has not been established.
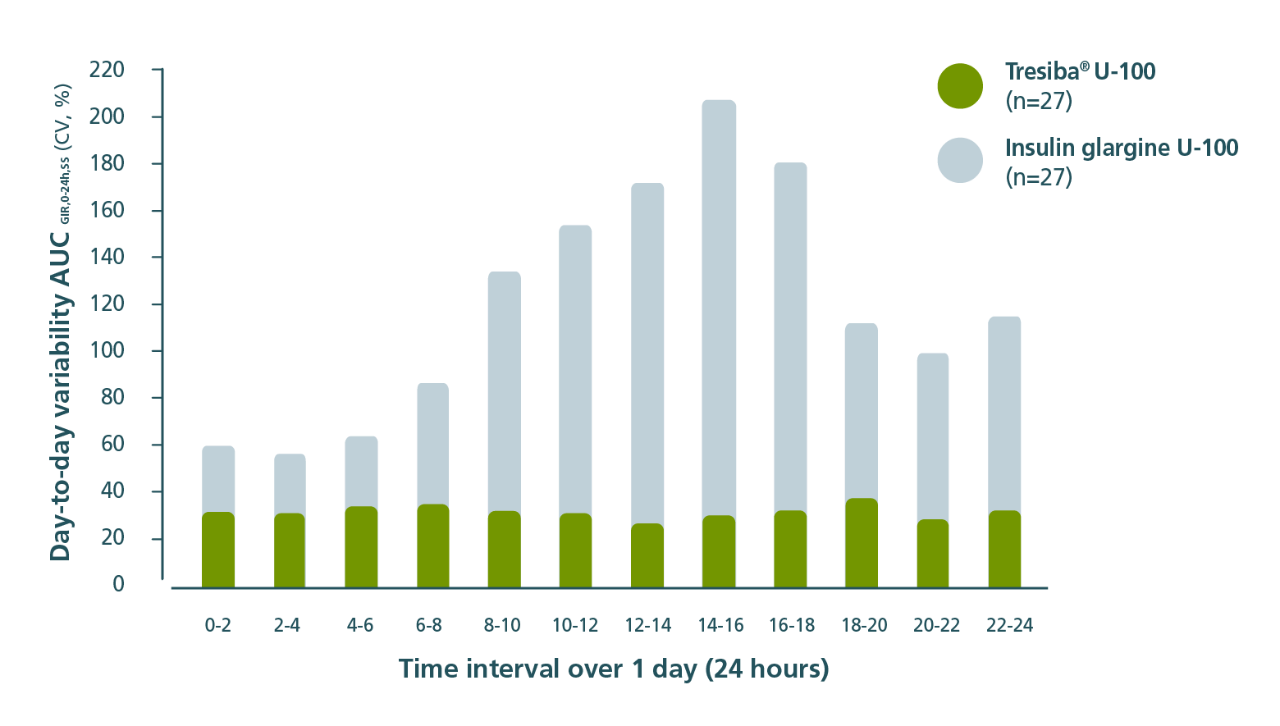
In a post hoc analysis
Tresiba® U-100 had less within-subject, day-to-day variability when evaluated every 2 hours vs insulin glargine U-1003
Calculated using the glucose infusion rate (GIR) profiles of adults with type 1 diabetes (P<0.0001)
2-hour intervals at steady state over the course of 24 hours
The clinical significance of these PK/PD differences has not been established.
Half-life
Tresiba®, a basal insulin, has a longer half-life than insulin glargine1,7-9,b

Tresiba®


Insulin glargine U-100

bThe mean half-life of other basal insulins: insulin glargine U-300: 19 hours4; NPH (Humulin N): 4.4 hours.9
c13.5-hour half-life for insulin glargine U-100 is based on 0.4 units/kg dose.
Study designs
The Heise, Hermanski, et al Study3
Population: Adults with type 1 diabetes.
Study design: Randomized, double-blind, parallel-group, single-center trial evaluating the within-subject, day-to-day variability and glucose-lowering effect of Tresiba® U-100 (n=27) vs insulin glargine U-100 (n=27) under steady-state conditions. Patients received Tresiba® U-100 or insulin glargine U-100 (0.4 units/kg) once daily for 12 days. The euglycemic clamp was performed on days 6, 9, and 12 of treatment, and blood samples were taken throughout each clamp period.
Primary endpoint: To evaluate the within-subject variability of the PD response between Tresiba® U-100 and insulin glargine U-100 based on the area under the glucose infusion rate curve (AUCGIR) during 1 dosing interval (0-24 hours) at steady state. The within-subject, day-to-day PD variability in glucose-lowering effect in the Tresiba® arm was 20% and in the insulin glargine U-100 arm was 82% at steady state.
Secondary PD endpoints: To investigate whether within-subject variability was consistent over 24 hours, the within-subject of AUCGIR in 2-hour intervals (AUCGIR,0-2h,SS’ AUCGIR,2-4h,SS’ AUCGIR,4-6h,SS’ AUCGIR,20-22h,SS’ AUCGIR,22-24h,SS) was analyzed in a post-hoc analysis.
The Heise, Korsatko, et al Study2
Population: Adults with type 1 diabetes or type 2 diabetes.
Study design: Post hoc analysis of 5 randomized, double-blind, single-center, phase 1 trials. Patients (n=195) received once-daily doses ranging from 0.4-0.8 U/kg and for 6-12 days, depending on the individual study.
Primary endpoint: Determining the duration and consistency of time to steady state Tresiba® U-100 following once-daily subcutaneous dosing in subjects of varying age and diabetes type.
AUCGIR,0-24h,SS=area under the GIR curve from 0 to 24 hours at steady state; CV=coefficient of variation; PK/PD=pharmacokinetic/pharmacodynamics.
Start your adult patients with diabetes on once-daily Tresiba® today
Important Safety Information for Tresiba®
Contraindications
- Tresiba® is contraindicated during episodes of hypoglycemia and in patients with hypersensitivity to insulin degludec or any of the excipients in Tresiba®
Warnings and Precautions
- Never Share a Tresiba® FlexTouch® Pen, Needle, or Syringe Between Patients, even if the needle is changed. Patients using Tresiba® vials should never share needles or syringes with another person. Sharing poses a risk for transmission of blood-borne pathogens.
- Hyperglycemia or Hypoglycemia with Changes in Insulin Regimen: Changes in an insulin regimen (e.g., insulin strength, manufacturer, type, or injection site or method of administration) may affect glycemic control and predispose to hypoglycemia or hyperglycemia. Repeated insulin injections into areas of lipodystrophy or localized cutaneous amyloidosis have been reported to result in hyperglycemia; and a sudden change in the injection site (to an unaffected area) has been reported to result in hypoglycemia. Make any changes to a patient’s insulin regimen under close medical supervision with increased frequency of blood glucose monitoring. Advise patients who have repeatedly injected into areas of lipodystrophy or localized cutaneous amyloidosis to change the injection site to unaffected areas and closely monitor for hypoglycemia. Adjustments in concomitant anti-diabetic treatment may be needed.
- Hypoglycemia: Hypoglycemia is the most common adverse reaction of insulin, including Tresiba®. Severe hypoglycemia can cause seizures, may be life-threatening or cause death. Hypoglycemia can impair concentration ability and reaction time; this may place the patient and others at risk in situations where these abilities are important (e.g., driving or operating other machinery). Hypoglycemia can happen suddenly and symptoms may differ in each patient and change over time in the same patient. Symptomatic awareness of hypoglycemia may be less pronounced in patients with longstanding diabetes, in patients with diabetic neuropathy, using drugs that block the sympathetic nervous system (e.g., beta-blockers) or who experience recurrent hypoglycemia. The long-acting effect of Tresiba® may delay recovery from hypoglycemia compared to shorter-acting insulins.
Risk Factors for Hypoglycemia: The risk of hypoglycemia generally increases with intensity of glycemic control. The risk of hypoglycemia after an injection is related to the duration of action of the insulin and, in general, is highest when the glucose lowering effect of the insulin is maximal. As with all insulins, the glucose lowering effect time course of Tresiba® may vary among different patients or at different times in the same patients and depends on many conditions, including the area of injection as well as the injection site blood supply and temperature. Other factors which may increase the risk of hypoglycemia include changes in meal pattern, changes in level of physical activity, or changes to concomitant drugs. Patients with renal or hepatic impairment may be at higher risk of hypoglycemia. Patients and caregivers must be educated to recognize and manage hypoglycemia. In patients at higher risk for hypoglycemia and patients who have reduced symptomatic awareness of hypoglycemia, increased frequency of blood glucose monitoring is recommended. - Hypoglycemia Due to Medication Errors: Accidental mix-ups between insulin products have been reported. To avoid medication errors between Tresiba® and other insulins, always instruct patients to always check the insulin label before each injection. To avoid dosing errors and potential overdose, never use a syringe to remove Tresiba® from the Tresiba® FlexTouch® disposable insulin prefilled pen.
- Hypersensitivity Reactions: Severe, life-threatening, generalized allergy, including anaphylaxis, can occur with insulins, including Tresiba®. If hypersensitivity reactions occur, discontinue Tresiba®; treat per standard of care and monitor until symptoms and signs resolve.
- Hypokalemia: All insulins, including Tresiba®, cause a shift in potassium from the extracellular to intracellular space, possibly leading to hypokalemia. Untreated hypokalemia may cause respiratory paralysis, ventricular arrhythmia, and death. Monitor potassium levels in patients at risk for hypokalemia and treat if indicated.
- Fluid Retention and Heart Failure with Concomitant Use of PPAR-gamma Agonists: Fluid retention and heart failure can occur with concomitant use of thiazolidinediones (TZDs), which are PPAR-gamma agonists, and insulin, including Tresiba®. Patients should be observed for signs and symptoms of heart failure. If heart failure occurs, dosage reduction or discontinuation of the TZD must be considered.
Adverse Reactions
- Adverse reactions commonly associated with Tresiba® are hypoglycemia, allergic reactions, injection site reactions, lipodystrophy, pruritus, rash, edema, and weight gain.
Drug Interactions
- There are certain drugs that may cause clinically significant drug interactions with Tresiba®.
- Drugs that may increase the risk of hypoglycemia: antidiabetic agents, ACE inhibitors, angiotensin II receptor blocking agents, disopyramide, fibrates, fluoxetine, monoamine oxidase inhibitors, pentoxifylline, pramlintide, salicylates, somatostatin analog (e.g., octreotide), sulfonamide antibiotics, GLP-1 receptor agonists, DPP-4 inhibitors, and SGLT-2 inhibitors
- Drugs that may decrease the blood glucose lowering effect: atypical antipsychotics (e.g., olanzapine and clozapine), corticosteroids, danazol, diuretics, estrogens, glucagon, isoniazid, niacin, oral contraceptives, phenothiazines, progestogens (e.g., in oral contraceptives), protease inhibitors, somatropin, sympathomimetic agents (e.g., albuterol, epinephrine, terbutaline), and thyroid hormones
- Drugs that may increase or decrease the blood glucose lowering effect: alcohol, beta-blockers, clonidine, lithium salts, and pentamidine
- Drugs that may blunt the signs and symptoms of hypoglycemia: beta-blockers, clonidine, guanethidine, and reserpine
Please click here for Tresiba® Prescribing Information.
Important Safety Information for Tresiba®
Contraindications
- Tresiba® is contraindicated during episodes of hypoglycemia and in patients with hypersensitivity to insulin degludec or any of the excipients in Tresiba®
Warnings and Precautions
- Never Share a Tresiba® FlexTouch® Pen, Needle, or Syringe Between Patients, even if the needle is changed. Patients using Tresiba® vials should never share needles or syringes with another person. Sharing poses a risk for transmission of blood-borne pathogens.
- Hyperglycemia or Hypoglycemia with Changes in Insulin Regimen: Changes in an insulin regimen (e.g., insulin strength, manufacturer, type, or injection site or method of administration) may affect glycemic control and predispose to hypoglycemia or hyperglycemia. Repeated insulin injections into areas of lipodystrophy or localized cutaneous amyloidosis have been reported to result in hyperglycemia; and a sudden change in the injection site (to an unaffected area) has been reported to result in hypoglycemia. Make any changes to a patient’s insulin regimen under close medical supervision with increased frequency of blood glucose monitoring. Advise patients who have repeatedly injected into areas of lipodystrophy or localized cutaneous amyloidosis to change the injection site to unaffected areas and closely monitor for hypoglycemia. Adjustments in concomitant anti-diabetic treatment may be needed.
- Hypoglycemia: Hypoglycemia is the most common adverse reaction of insulin, including Tresiba®. Severe hypoglycemia can cause seizures, may be life-threatening or cause death. Hypoglycemia can impair concentration ability and reaction time; this may place the patient and others at risk in situations where these abilities are important (e.g., driving or operating other machinery). Hypoglycemia can happen suddenly and symptoms may differ in each patient and change over time in the same patient. Symptomatic awareness of hypoglycemia may be less pronounced in patients with longstanding diabetes, in patients with diabetic neuropathy, using drugs that block the sympathetic nervous system (e.g., beta-blockers) or who experience recurrent hypoglycemia. The long-acting effect of Tresiba® may delay recovery from hypoglycemia compared to shorter-acting insulins.
Risk Factors for Hypoglycemia: The risk of hypoglycemia generally increases with intensity of glycemic control. The risk of hypoglycemia after an injection is related to the duration of action of the insulin and, in general, is highest when the glucose lowering effect of the insulin is maximal. As with all insulins, the glucose lowering effect time course of Tresiba® may vary among different patients or at different times in the same patients and depends on many conditions, including the area of injection as well as the injection site blood supply and temperature. Other factors which may increase the risk of hypoglycemia include changes in meal pattern, changes in level of physical activity, or changes to concomitant drugs. Patients with renal or hepatic impairment may be at higher risk of hypoglycemia. Patients and caregivers must be educated to recognize and manage hypoglycemia. In patients at higher risk for hypoglycemia and patients who have reduced symptomatic awareness of hypoglycemia, increased frequency of blood glucose monitoring is recommended. - Hypoglycemia Due to Medication Errors: Accidental mix-ups between insulin products have been reported. To avoid medication errors between Tresiba® and other insulins, always instruct patients to always check the insulin label before each injection. To avoid dosing errors and potential overdose, never use a syringe to remove Tresiba® from the Tresiba® FlexTouch® disposable insulin prefilled pen.
- Hypersensitivity Reactions: Severe, life-threatening, generalized allergy, including anaphylaxis, can occur with insulins, including Tresiba®. If hypersensitivity reactions occur, discontinue Tresiba®; treat per standard of care and monitor until symptoms and signs resolve.
- Hypokalemia: All insulins, including Tresiba®, cause a shift in potassium from the extracellular to intracellular space, possibly leading to hypokalemia. Untreated hypokalemia may cause respiratory paralysis, ventricular arrhythmia, and death. Monitor potassium levels in patients at risk for hypokalemia and treat if indicated.
- Fluid Retention and Heart Failure with Concomitant Use of PPAR-gamma Agonists: Fluid retention and heart failure can occur with concomitant use of thiazolidinediones (TZDs), which are PPAR-gamma agonists, and insulin, including Tresiba®. Patients should be observed for signs and symptoms of heart failure. If heart failure occurs, dosage reduction or discontinuation of the TZD must be considered.
Adverse Reactions
- Adverse reactions commonly associated with Tresiba® are hypoglycemia, allergic reactions, injection site reactions, lipodystrophy, pruritus, rash, edema, and weight gain.
Drug Interactions
- There are certain drugs that may cause clinically significant drug interactions with Tresiba®.
- Drugs that may increase the risk of hypoglycemia: antidiabetic agents, ACE inhibitors, angiotensin II receptor blocking agents, disopyramide, fibrates, fluoxetine, monoamine oxidase inhibitors, pentoxifylline, pramlintide, salicylates, somatostatin analog (e.g., octreotide), sulfonamide antibiotics, GLP-1 receptor agonists, DPP-4 inhibitors, and SGLT-2 inhibitors
- Drugs that may decrease the blood glucose lowering effect: atypical antipsychotics (e.g., olanzapine and clozapine), corticosteroids, danazol, diuretics, estrogens, glucagon, isoniazid, niacin, oral contraceptives, phenothiazines, progestogens (e.g., in oral contraceptives), protease inhibitors, somatropin, sympathomimetic agents (e.g., albuterol, epinephrine, terbutaline), and thyroid hormones
- Drugs that may increase or decrease the blood glucose lowering effect: alcohol, beta-blockers, clonidine, lithium salts, and pentamidine
- Drugs that may blunt the signs and symptoms of hypoglycemia: beta-blockers, clonidine, guanethidine, and reserpine
Please click here for Tresiba® Prescribing Information.
References:
- Tresiba [package insert]. Plainsboro, NJ: Novo Nordisk Inc.
- Heise T, Korsatko S, Nosek L, et al. J Diabetes. 2016;8(1):132-138.
- Heise T, Hermanski L, Nosek L, Feldman A, Rasmussen S, Haahr H. Diabetes Obes Metab. 2012;14(9):859-864.
- Becker RHA, Dahmen R, Bergmann K, Lehmann A, Jax T, Heise T. Diabetes Care. 2015;38(4):637-643.
- Toujeo [package insert]. Bridgewater, NJ: sanofi-aventis US LLC; May 2025.
- Lantus [package insert]. Bridgewater, NJ: sanofi-aventis US LLC; May 2025.
- Basaglar [package insert]. Indianapolis, IN: Lilly USA LLC; July 2021.
- Heise T, Hövelmann U, Nosek L, et al. Expert Opin Drug Metab Toxicol. 2015;11(8):1193-1201.
- Humulin N [package insert]. Indianapolis, IN: Eli Lilly and Company; June 2022.