
RYBELSUS® (semaglutide)—GLP-1 RA in a once-daily pill1
Explore the efficacy of the first FDA-approved semaglutide in a pill for adult patients with type 2 diabetes.1
Indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes.


See how RYBELSUS® measured up vs multiple treatments for type 2 diabetes in the PIONEER phase 3 clinical trial program
Bring A1C down with the proven efficacy of RYBELSUS®
26-WEEK RESULTS
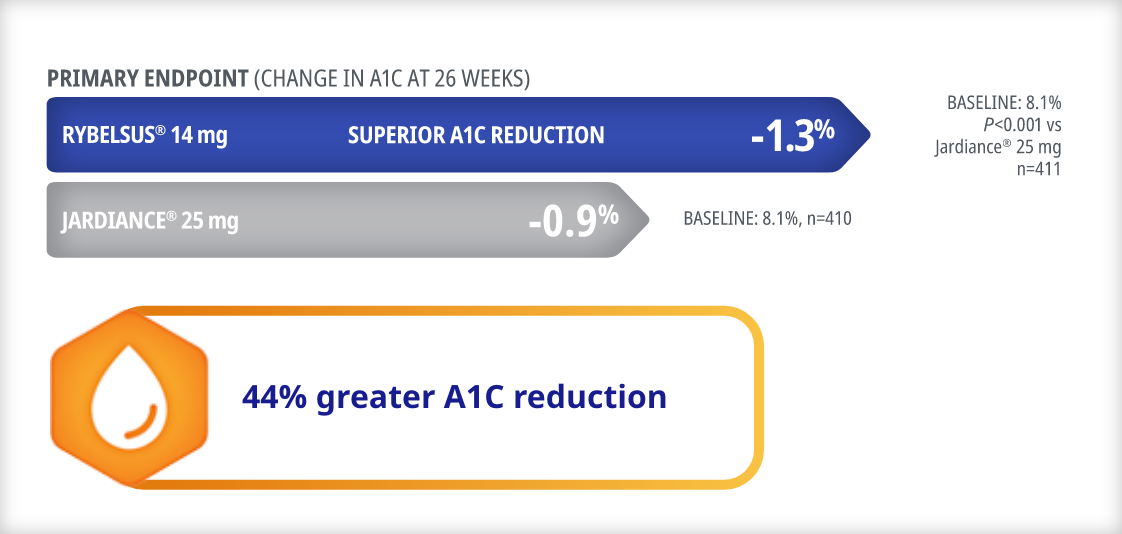
Superior A1C reduction vs Jardiance® (empagliflozin)1
Superior A1C control vs Jardiance®1,2*
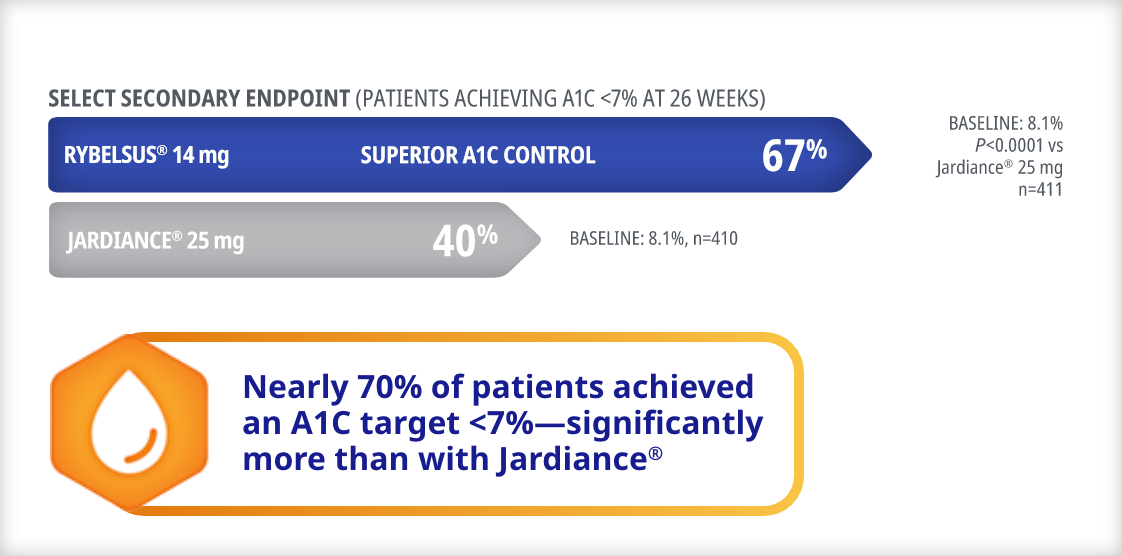
PIONEER 2 study design1,2
In an open-label trial with a primary endpoint of mean change in A1C from baseline to 26 weeks, 822 adult patients with type 2 diabetes on metformin were randomized to RYBELSUS® 14 mg (n=411) or Jardiance® 25 mg (n=410), both once daily.
- Confirmatory secondary endpoint: Mean change in body weight from baseline to 26 weeks
- Secondary endpoints included: Proportion of patients achieving A1C <7% at Week 26 and 52, and mean changes from baseline to Week 52 in A1C and body weight
*Endpoint not adjusted for multiplicity.
RYBELSUS®: A1C reduction demonstrated at 52 weeks
Statistically significant A1C reduction vs Jardiance®2*

Statistically significant A1C control vs Jardiance®2*


PIONEER 2 study design1,2
In an open-label trial with a primary endpoint of mean change in A1C from baseline to 26 weeks, 822 adult patients with type 2 diabetes on metformin were randomized to RYBELSUS® 14 mg (n=411) or Jardiance® 25 mg (n=410), both once daily.
- Confirmatory secondary endpoint: Mean change in body weight from baseline to 26 weeks
- Secondary endpoints included: Proportion of patients achieving A1C <7% at Week 26 and 52, and mean changes from baseline to Week 52 in A1C and body weight
*Endpoint not adjusted for multiplicity.
RYBELSUS® demonstrated weight loss
26-WEEK RESULTS
Comparable weight reduction with RYBELSUS® 14 mg vs Jardiance®1,3
RYBELSUS® is not indicated for weight loss.
Mean change in body weight from baseline to Week 26 was a confirmatory secondary endpoint.

PIONEER 2 study design1,3
In an open-label trial with a primary endpoint of mean change in A1C from baseline to 26 weeks, 822 adult patients with type 2 diabetes on metformin were randomized to RYBELSUS® 14 mg (n=411) or Jardiance® 25 mg (n=410), both once daily.
- Confirmatory secondary endpoint: Mean change in body weight from baseline to 26 weeks
- Secondary endpoints included: Proportion of patients achieving A1C <7% at Week 26 and 52, and mean changes from baseline to Week 52 in A1C and body weight
RYBELSUS®: Sustainable weight loss at 52 weeks1,3
RYBELSUS® is not indicated for weight loss.
Mean change in body weight from baseline to Week 52 was a secondary endpoint.*
Comparable weight reduction with RYBELSUS® 14 mg vs Jardiance®

PIONEER 2 study design1,3
In an open-label trial with a primary endpoint of mean change in A1C from baseline to 26 weeks, 822 adult patients with type 2 diabetes on metformin were randomized to RYBELSUS® 14 mg (n=411) or Jardiance® 25 mg (n=410), both once daily.
- Confirmatory secondary endpoint: Mean change in body weight from baseline to 26 weeks
- Secondary endpoints included: Proportion of patients achieving A1C <7% at Week 26 and 52, and mean changes from baseline to Week 52 in A1C and body weight
*Endpoint not adjusted for multiplicity.
A1C=glycated hemoglobin; DPP-4i=dipeptidyl peptidase-4 inhibitor; ETD=estimated treatment difference; GLP-1 RA=glucagon-like peptide-1 receptor agonist; MET=metformin; SGLT-2i=sodium-glucose cotransporter-2 inhibitor.
Bring A1C down with the proven efficacy of RYBELSUS®
26-WEEK RESULTS
Superior A1C reduction vs Januvia® (sitagliptin)1

63% greater A1C reduction with RYBELSUS® 14 mg vs Januvia®
Superior A1C control vs Januvia®1,4*

*Endpoint not adjusted for multiplicity.
1.7x more patients achieved an A1C target <7% with RYBELSUS® 14 mg vs Januvia®
PIONEER 3 study design1,4
In a double-blind, double-dummy trial with a primary endpoint of mean change in A1C from baseline to 26 weeks, 1864 adult patients with type 2 diabetes on metformin alone or metformin with a sulfonylurea were randomized to RYBELSUS® 3 mg (n=466), RYBELSUS® 7 mg (n=465), RYBELSUS® 14 mg (n=465), or Januvia® 100 mg (n=467), all once daily.
- Confirmatory secondary endpoint: Mean change in body weight from baseline to 26 weeks
- Secondary endpoints included: Proportion of patients achieving A1C <7% at Week 26 and 52, and mean changes from baseline to Week 52 in A1C and body weight
RYBELSUS®: Sustainable A1C reduction demonstrated at 52 weeks
Statistically significant A1C reduction vs Januvia®4,5*

Statistically significant A1C control vs Januvia®4,5*


PIONEER 3 study design1,4
In a double-blind, double-dummy trial with a primary endpoint of mean change in A1C from baseline to 26 weeks, 1864 adult patients with type 2 diabetes on metformin alone or metformin with a sulfonylurea were randomized to RYBELSUS® 3 mg (n=466), RYBELSUS® 7 mg (n=465), RYBELSUS® 14 mg (n=465), or Januvia® 100 mg (n=467), all once daily.
- Confirmatory secondary endpoint: Mean change in body weight from baseline to 26 weeks
- Secondary endpoints included: Proportion of patients achieving A1C <7% at Week 26 and 52, and mean changes from baseline to Week 52 in A1C and body weight
*Endpoint not adjusted for multiplicity.
RYBELSUS® demonstrated weight loss
26-WEEK RESULTS
Superior weight reductions with RYBELSUS® 14 mg and 7 mg vs Januvia®1,4
RYBELSUS® is not indicated for weight loss.
Mean change in body weight from baseline to Week 26 was a confirmatory secondary endpoint.

PIONEER 3 study design1,4
In a double-blind, double-dummy trial with a primary endpoint of mean change in A1C from baseline to 26 weeks, 1864 adult patients with type 2 diabetes on metformin alone or metformin with a sulfonylurea were randomized to RYBELSUS® 3 mg (n=466), RYBELSUS® 7 mg (n=465), RYBELSUS® 14 mg (n=465), or Januvia® 100 mg (n=467), all once daily.
- Confirmatory secondary endpoint: Mean change in body weight from baseline to 26 weeks
- Secondary endpoints included: Proportion of patients achieving A1C <7% at Week 26 and 52, and mean changes from baseline to Week 52 in A1C and body weight
RYBELSUS®: Sustainable weight loss at 52 weeks4,5
RYBELSUS® is not indicated for weight loss.
Mean change in body weight from baseline to Week 52 was a secondary endpoint.*
Statistically significant vs Januvia® 100 mg

PIONEER 3 study design1,4
In a double-blind, double-dummy trial with a primary endpoint of mean change in A1C from baseline to 26 weeks, 1864 adult patients with type 2 diabetes on metformin alone or metformin with a sulfonylurea were randomized to RYBELSUS® 3 mg (n=466), RYBELSUS® 7 mg (n=465), RYBELSUS® 14 mg (n=465), or Januvia® 100 mg (n=467), all once daily.
- Confirmatory secondary endpoint: Mean change in body weight from baseline to 26 weeks
- Secondary endpoints included: Proportion of patients achieving A1C <7% at Week 26 and 52, and mean changes from baseline to Week 52 in A1C and body weight
*Endpoint not adjusted for multiplicity.
A1C=glycated hemoglobin; DPP-4i=dipeptidyl peptidase-4 inhibitor; ETD=estimated treatment difference; MET=metformin; SGLT-2i=sodium-glucose cotransporter-2 inhibitor.
Bring A1C down with the proven efficacy of RYBELSUS®
Comparable A1C reduction vs liraglutide 1.8 mg1,6

Comparable A1C control vs liraglutide 1.8 mg1,6*

*Endpoint not adjusted for multiplicity.
Nearly 70% of the patients achieved an A1C of less than 7%—comparable to liraglutide 1.8 mg
PIONEER 4 study design1,6
In a double-blind, double-dummy trial with a primary endpoint of mean change in A1C from baseline to 26 weeks, 711 adult patients with type 2 diabetes on metformin alone or metformin with an SGLT-2i were randomized to RYBELSUS® 14 mg (n=285), liraglutide 1.8 mg subcutaneous injection (n=284), or placebo (n=142), all once daily.
- Confirmatory secondary endpoint: Mean change in body weight from baseline to 26 weeks
- Select secondary endpoint: Proportion of patients achieving A1C <7% at Week 26
A1C=glycated hemoglobin; DPP-4i=dipeptidyl peptidase-4 inhibitor; SGLT-2i=sodium-glucose cotransporter-2 inhibitor.
RYBELSUS® demonstrated weight loss
Superior weight reductions with RYBELSUS® 14 mg vs liraglutide 1.8 mg1,6
RYBELSUS® is not indicated for weight loss.
Mean change in body weight from baseline to Week 26 was a confirmatory secondary endpoint.

42% greater weight reduction with RYBELSUS® 14 mg than liraglutide 1.8 mg
PIONEER 4 study design1,6
In a double-blind, double-dummy trial with a primary endpoint of mean change in A1C from baseline to 26 weeks, 711 adult patients with type 2 diabetes on metformin alone or metformin with an SGLT-2i were randomized to RYBELSUS® 14 mg (n=285), liraglutide 1.8 mg subcutaneous injection (n=284), or placebo (n=142), all once daily.
- Confirmatory secondary endpoint: Mean change in body weight from baseline to 26 weeks
- Select secondary endpoint: Proportion of patients achieving A1C <7% at Week 26
A1C=glycated hemoglobin; DPP-4i=dipeptidyl peptidase-4 inhibitor; ETD=estimated treatment difference; GLP-1 RA=glucagon-like peptide-1 receptor agonist; MET=metformin; SGLT-2i=sodium-glucose cotransporter-2 inhibitor.
Explore the CVOT study for RYBELSUS®
PIONEER 6: cardiovascular safety6,7
Study design: In a double-blind trial, 3183 adult patients with inadequately controlled type 2 diabetes at high CV risk (≥50 years of age with CVD or CKD, or ≥60 with at least 1 CV risk factor) were randomized to RYBELSUS® 14 mg (n=1591) or placebo (n=1592), both once daily and in addition to standard of care for a median observation time of 16 months. Background antidiabetic therapy included OADs and/or insulin. Patients could also be treatment naïve. Most patients were also on antihypertensive therapies, lipid-lowering therapies, and antiplatelet or antithrombotic therapy.
The primary endpoint was the time to first occurrence of MACE, which included CV death, nonfatal myocardial infarction, or nonfatal stroke.
Secondary endpoints included time from randomization to the first occurrence of an expanded composite outcome consisting of the primary outcome plus unstable angina resulting in hospitalization or heart failure resulting in hospitalization or a composite of death from any cause, nonfatal myocardial infarction, or nonfatal stroke.
CKD=chronic kidney disease; CV=cardiovascular; CVOT=cardiovascular outcomes trial; MACE=major adverse cardiovascular event; OADs=oral antidiabetic drugs.
Meet a patient ready for RYBELSUS®
Find out why Cynthia would benefit from a change in her T2D treatment regimen
Actor portrayal of a
hypothetical patient


Important Safety Information for RYBELSUS®
WARNING: RISK OF THYROID C-CELL TUMORS
- In rodents, semaglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures. It is unknown whether RYBELSUS® causes thyroid C-cell tumors, including medullary thyroid carcinoma (MTC), in humans as human relevance of semaglutide-induced rodent thyroid C-cell tumors has not been determined
- RYBELSUS® is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). Counsel patients regarding the potential risk for MTC with the use of RYBELSUS® and inform them of symptoms of thyroid tumors (e.g. a mass in the neck, dysphagia, dyspnea, persistent hoarseness). Routine monitoring of serum calcitonin or using thyroid ultrasound is of uncertain value for early detection of MTC in patients treated with RYBELSUS®
Contraindications
- RYBELSUS® is contraindicated in patients with a personal or family history of medullary thyroid carcinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2), and in patients with a prior serious hypersensitivity reaction to semaglutide or to any of the excipients in RYBELSUS®. Serious hypersensitivity reactions including anaphylaxis and angioedema have been reported with RYBELSUS®
Warnings and Precautions
- Risk of Thyroid C-Cell Tumors: Patients should be further evaluated if serum calcitonin is measured and found to be elevated or thyroid nodules are noted on physical examination or neck imaging
- Acute Pancreatitis: Acute pancreatitis, including fatal and non-fatal hemorrhagic or necrotizing pancreatitis, has been observed in patients treated with GLP-1 receptor agonists, including RYBELSUS®. Observe patients carefully for signs and symptoms of acute pancreatitis which may include persistent or severe abdominal pain (sometimes radiating to the back), nausea or vomiting. If pancreatitis is suspected, discontinue RYBELSUS® and initiate appropriate management
- Diabetic Retinopathy Complications: In a pooled analysis of glycemic control trials with RYBELSUS®, patients reported diabetic retinopathy related adverse reactions during the trial (4.2% with RYBELSUS® and 3.8% with comparator). In a 2-year trial with semaglutide injection involving patients with type 2 diabetes and high cardiovascular risk, more events of diabetic retinopathy complications occurred in patients treated with semaglutide injection (3.0%) compared to placebo (1.8%). The absolute risk increase for diabetic retinopathy complications was larger among patients with a history of diabetic retinopathy at baseline than among patients without a known history of diabetic retinopathy.
Rapid improvement in glucose control has been associated with a temporary worsening of diabetic retinopathy. Patients with a history of diabetic retinopathy should be monitored for progression of diabetic retinopathy - Hypoglycemia: Patients receiving RYBELSUS® in combination with an insulin secretagogue (e.g., sulfonylurea) or insulin may have an increased risk of hypoglycemia, including severe hypoglycemia. Inform patients using these concomitant medications of the risk of hypoglycemia and educate them on the signs and symptoms of hypoglycemia
- Acute Kidney Injury Due to Volume Depletion: There have been postmarketing reports of acute kidney injury in some cases requiring hemodialysis, in patients treated with semaglutide. The majority of the reported events occurred in patients who had experienced gastrointestinal reactions leading to dehydration such as nausea, vomiting, or diarrhea. Monitor renal function in patients reporting adverse reactions to RYBELSUS® that could lead to volume depletion, especially during initiation and escalation of RYBELSUS®
- Severe Gastrointestinal Adverse Reactions: Use of RYBELSUS® has been associated with gastrointestinal adverse reactions, sometimes severe. In clinical trials, severe gastrointestinal adverse reactions were reported more frequently among patients receiving RYBELSUS® (7 mg 0.6%, 14 mg 2%) than placebo (0.3%). RYBELSUS® is not recommended in patients with severe gastroparesis
- Hypersensitivity: Serious hypersensitivity reactions (e.g., anaphylaxis, angioedema) have been reported in patients treated with RYBELSUS®. If hypersensitivity reactions occur, discontinue use of RYBELSUS®, treat promptly per standard of care, and monitor until signs and symptoms resolve. Use caution in a patient with a history of angioedema or anaphylaxis with another GLP-1 receptor agonist
- Acute Gallbladder Disease: Acute events of gallbladder disease such as cholelithiasis or cholecystitis have been reported in GLP-1 receptor agonist trials and postmarketing. In placebo-controlled trials to improve glycemic control, cholelithiasis was reported in 1% of patients treated with RYBELSUS® 7 mg. In a 4-year cardiovascular outcomes trial (Trial 7), cholelithiasis was reported in 1.1% of patients treated with RYBELSUS® 14 mg and in 0.9% of placebo-treated patients. In Trial 7, cholecystitis was reported in 1.1% treated with RYBELSUS® 14 mg and in 0.7% of placebo-treated patients. If cholelithiasis or cholecystitis is suspected, gallbladder studies and appropriate clinical follow-up are indicated
- Pulmonary Aspiration During General Anesthesia or Deep Sedation: RYBELSUS® delays gastric emptying. There have been rare postmarketing reports of pulmonary aspiration in patients receiving GLP-1 receptor agonists undergoing elective surgeries or procedures requiring general anesthesia or deep sedation who had residual gastric contents despite reported adherence to preoperative fasting recommendations. Instruct patients to inform healthcare providers prior to any planned surgeries or procedures if they are taking RYBELSUS®
Adverse Reactions
- Most common adverse reactions (incidence ≥5%) are nausea, abdominal pain, diarrhea, decreased appetite, vomiting and constipation
Drug Interactions
- RYBELSUS® stimulates insulin release in the presence of elevated blood glucose concentrations. When initiating RYBELSUS®, consider reducing the dose of concomitantly administered insulin secretagogue (such as sulfonylureas) or insulin to reduce the risk of hypoglycemia
- RYBELSUS® delays gastric emptying and has the potential to impact the absorption of other oral medications. Closely follow RYBELSUS® administration instructions when coadministering with other oral medications and consider increased monitoring for medications with a narrow therapeutic index, such as levothyroxine
Use in Specific Populations
- Pregnancy: Available data with RYBELSUS® are not sufficient to determine a drug associated risk for major birth defects, miscarriage, or other adverse maternal or fetal outcomes. Discontinue RYBELSUS® in women at least 2 months before a planned pregnancy due to the long washout period for semaglutide
- Lactation: A clinical lactation study reported semaglutide concentrations below the lower limit of quantification in human breast milk. However, salcaprozate sodium (SNAC) and/or its metabolites are present in human milk. Because of the unknown potential for serious adverse reactions in the breastfed infant due to the possible accumulation of SNAC, an absorption enhancer for RYBELSUS®, and because there are alternative formulations of semaglutide that do not contain SNAC that can be used during lactation, advise patients that breastfeeding is not recommended during treatment with RYBELSUS®
Please click here for RYBELSUS® Prescribing Information, including Boxed Warning.
Indication and Usage
RYBELSUS® (semaglutide) tablets 7 mg or 14 mg is indicated:
- as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes
- to reduce the risk of major adverse cardiovascular events (cardiovascular death, non-fatal myocardial infarction or non-fatal stroke) in adults with type 2 diabetes mellitus who are at high risk for these events
Important Safety Information for RYBELSUS®
WARNING: RISK OF THYROID C-CELL TUMORS
- In rodents, semaglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures. It is unknown whether RYBELSUS® causes thyroid C-cell tumors, including medullary thyroid carcinoma (MTC), in humans as human relevance of semaglutide-induced rodent thyroid C-cell tumors has not been determined
- RYBELSUS® is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). Counsel patients regarding the potential risk for MTC with the use of RYBELSUS® and inform them of symptoms of thyroid tumors (e.g. a mass in the neck, dysphagia, dyspnea, persistent hoarseness). Routine monitoring of serum calcitonin or using thyroid ultrasound is of uncertain value for early detection of MTC in patients treated with RYBELSUS®
Important Safety Information for RYBELSUS®
WARNING: RISK OF THYROID C-CELL TUMORS
- In rodents, semaglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures. It is unknown whether RYBELSUS® causes thyroid C-cell tumors, including medullary thyroid carcinoma (MTC), in humans as human relevance of semaglutide-induced rodent thyroid C-cell tumors has not been determined
- RYBELSUS® is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). Counsel patients regarding the potential risk for MTC with the use of RYBELSUS® and inform them of symptoms of thyroid tumors (e.g. a mass in the neck, dysphagia, dyspnea, persistent hoarseness). Routine monitoring of serum calcitonin or using thyroid ultrasound is of uncertain value for early detection of MTC in patients treated with RYBELSUS®
Contraindications
- RYBELSUS® is contraindicated in patients with a personal or family history of medullary thyroid carcinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2), and in patients with a prior serious hypersensitivity reaction to semaglutide or to any of the excipients in RYBELSUS®. Serious hypersensitivity reactions including anaphylaxis and angioedema have been reported with RYBELSUS®
Warnings and Precautions
- Risk of Thyroid C-Cell Tumors: Patients should be further evaluated if serum calcitonin is measured and found to be elevated or thyroid nodules are noted on physical examination or neck imaging
- Acute Pancreatitis: Acute pancreatitis, including fatal and non-fatal hemorrhagic or necrotizing pancreatitis, has been observed in patients treated with GLP-1 receptor agonists, including RYBELSUS®. Observe patients carefully for signs and symptoms of acute pancreatitis which may include persistent or severe abdominal pain (sometimes radiating to the back), nausea or vomiting. If pancreatitis is suspected, discontinue RYBELSUS® and initiate appropriate management
- Diabetic Retinopathy Complications: In a pooled analysis of glycemic control trials with RYBELSUS®, patients reported diabetic retinopathy related adverse reactions during the trial (4.2% with RYBELSUS® and 3.8% with comparator). In a 2-year trial with semaglutide injection involving patients with type 2 diabetes and high cardiovascular risk, more events of diabetic retinopathy complications occurred in patients treated with semaglutide injection (3.0%) compared to placebo (1.8%). The absolute risk increase for diabetic retinopathy complications was larger among patients with a history of diabetic retinopathy at baseline than among patients without a known history of diabetic retinopathy.
Rapid improvement in glucose control has been associated with a temporary worsening of diabetic retinopathy. Patients with a history of diabetic retinopathy should be monitored for progression of diabetic retinopathy - Hypoglycemia: Patients receiving RYBELSUS® in combination with an insulin secretagogue (e.g., sulfonylurea) or insulin may have an increased risk of hypoglycemia, including severe hypoglycemia. Inform patients using these concomitant medications of the risk of hypoglycemia and educate them on the signs and symptoms of hypoglycemia
- Acute Kidney Injury Due to Volume Depletion: There have been postmarketing reports of acute kidney injury in some cases requiring hemodialysis, in patients treated with semaglutide. The majority of the reported events occurred in patients who had experienced gastrointestinal reactions leading to dehydration such as nausea, vomiting, or diarrhea. Monitor renal function in patients reporting adverse reactions to RYBELSUS® that could lead to volume depletion, especially during initiation and escalation of RYBELSUS®
- Severe Gastrointestinal Adverse Reactions: Use of RYBELSUS® has been associated with gastrointestinal adverse reactions, sometimes severe. In clinical trials, severe gastrointestinal adverse reactions were reported more frequently among patients receiving RYBELSUS® (7 mg 0.6%, 14 mg 2%) than placebo (0.3%). RYBELSUS® is not recommended in patients with severe gastroparesis
- Hypersensitivity: Serious hypersensitivity reactions (e.g., anaphylaxis, angioedema) have been reported in patients treated with RYBELSUS®. If hypersensitivity reactions occur, discontinue use of RYBELSUS®, treat promptly per standard of care, and monitor until signs and symptoms resolve. Use caution in a patient with a history of angioedema or anaphylaxis with another GLP-1 receptor agonist
- Acute Gallbladder Disease: Acute events of gallbladder disease such as cholelithiasis or cholecystitis have been reported in GLP-1 receptor agonist trials and postmarketing. In placebo-controlled trials to improve glycemic control, cholelithiasis was reported in 1% of patients treated with RYBELSUS® 7 mg. In a 4-year cardiovascular outcomes trial (Trial 7), cholelithiasis was reported in 1.1% of patients treated with RYBELSUS® 14 mg and in 0.9% of placebo-treated patients. In Trial 7, cholecystitis was reported in 1.1% treated with RYBELSUS® 14 mg and in 0.7% of placebo-treated patients. If cholelithiasis or cholecystitis is suspected, gallbladder studies and appropriate clinical follow-up are indicated
- Pulmonary Aspiration During General Anesthesia or Deep Sedation: RYBELSUS® delays gastric emptying. There have been rare postmarketing reports of pulmonary aspiration in patients receiving GLP-1 receptor agonists undergoing elective surgeries or procedures requiring general anesthesia or deep sedation who had residual gastric contents despite reported adherence to preoperative fasting recommendations. Instruct patients to inform healthcare providers prior to any planned surgeries or procedures if they are taking RYBELSUS®
Adverse Reactions
- Most common adverse reactions (incidence ≥5%) are nausea, abdominal pain, diarrhea, decreased appetite, vomiting and constipation
Drug Interactions
- RYBELSUS® stimulates insulin release in the presence of elevated blood glucose concentrations. When initiating RYBELSUS®, consider reducing the dose of concomitantly administered insulin secretagogue (such as sulfonylureas) or insulin to reduce the risk of hypoglycemia
- RYBELSUS® delays gastric emptying and has the potential to impact the absorption of other oral medications. Closely follow RYBELSUS® administration instructions when coadministering with other oral medications and consider increased monitoring for medications with a narrow therapeutic index, such as levothyroxine
Use in Specific Populations
- Pregnancy: Available data with RYBELSUS® are not sufficient to determine a drug associated risk for major birth defects, miscarriage, or other adverse maternal or fetal outcomes. Discontinue RYBELSUS® in women at least 2 months before a planned pregnancy due to the long washout period for semaglutide
- Lactation: A clinical lactation study reported semaglutide concentrations below the lower limit of quantification in human breast milk. However, salcaprozate sodium (SNAC) and/or its metabolites are present in human milk. Because of the unknown potential for serious adverse reactions in the breastfed infant due to the possible accumulation of SNAC, an absorption enhancer for RYBELSUS®, and because there are alternative formulations of semaglutide that do not contain SNAC that can be used during lactation, advise patients that breastfeeding is not recommended during treatment with RYBELSUS®
Please click here for RYBELSUS® Prescribing Information, including Boxed Warning.
Indication and Usage
RYBELSUS® (semaglutide) tablets 7 mg or 14 mg is indicated:
- as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes
- to reduce the risk of major adverse cardiovascular events (cardiovascular death, non-fatal myocardial infarction or non-fatal stroke) in adults with type 2 diabetes mellitus who are at high risk for these events
References:
- RYBELSUS® [package insert]. Plainsboro, NJ: Novo Nordisk Inc.
- Rodbard HW, Rosenstock J, Canani LH, et al. Oral semaglutide versus empagliflozin in patients with type 2 diabetes uncontrolled on metformin: the PIONEER 2 trial. Diabetes Care. 2019;42(12):2272-2281.
- Rosenstock J, Allison D, Birkenfeld AL, et al. Effect of additional oral semaglutide vs sitagliptin on glycated hemoglobin in adults with type 2 diabetes uncontrolled with metformin alone or with sulfonylurea: the PIONEER 3 randomized clinical trial. JAMA. 2019;321(15):1466-1480.
- Data on file. Novo Nordisk Inc; November 2018.
- Pratley R, Amod A, Hoff ST, et al. Oral semaglutide versus subcutaneous liraglutide and placebo in type 2 diabetes (PIONEER 4): a randomised, double-blind, phase 3a trial. Lancet. 2019;394(10192):39-50.
- Bain SC, Mosenzon O, Arechavaleta R, et al. Cardiovascular safety of oral semaglutide in patients with type 2 diabetes: rationale, design and patient baseline characteristics for the PIONEER 6 trial. Diabetes Obes Metab. 2019;21(3):499-508.
- Husain M, Birkenfeld AL, Donsmark M, et al. Oral semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2019;381(9):841-851.