
In addition to diet and exercise, to reduce the risk of MACE (CV death, non-fatal MI, or non-fatal stroke) in adults with established CVD and either overweight or obesity and for chronic weight management in adults with obesity or overweight with at least one weight-related comorbidity. Click for Limitations of Use.

Actor portrayals.
For adults with established CVD and either overweight or obesity, along with diet and exercise
Shown to reduce the risk of life-threatening CV events in clinical trials and backed by real-world evidence1-3
#1 prescribed medication among cardiologists in the US, indicated to reduce cardiovascular risk and treat obesity
For adults with overweight or obesity with at least one weight-related comorbidity, along with diet and exercise
Proven significant, sustained weight loss across both pen and pill1
SELECT CVOT Study
SELECT, a landmark study: The largest CVOT ever completed for patients with established CVD and obesity1,2,4
MACE risk reduction was evaluated on top of CV standard of care1*
Patient population
17,604
patients without diabetes
17,061 (~97%) completed the trial1,2†
Patient enrollment: October 2018-March 2021
It took Novo Nordisk 4.5 years to conduct this trial
Key Inclusion Criteria
Adults: ≥45 years
BMI: ≥27 kg/m2
Established CVD:
• Prior MI
• Prior stroke
• PAD


Treatment arms1,2

Event-driven superiority trial: 1,225 accrued events
Median duration of follow-up: 41.8 months

Primary composite end point
Time from randomized to
first occurrence of MACE1,2
Assessed regardless of change in weight
What could life-saving outcomes mean for your patients?
CV standard-of-care treatments at baseline included1,2‡:
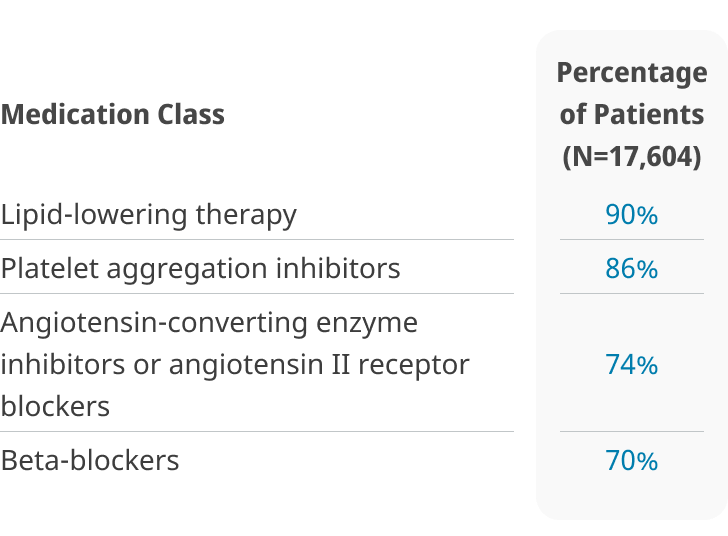
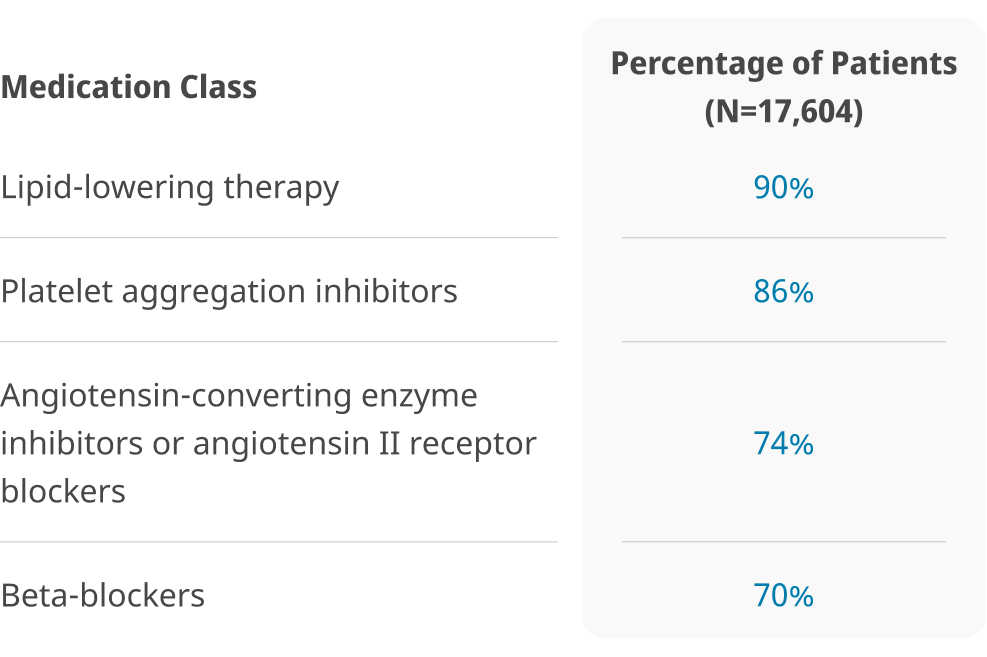
Medication Class
Lipid-lowering therapy
Platelet aggregation inhibitors
Angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers
Beta-blockers
Percentage of Patients (N=17,604)
90%
86%
74%
70%
Throughout the trial, CV therapies could be adjusted at investigator discretion according to current standard of care1
Baseline cardiometabolic parameters1
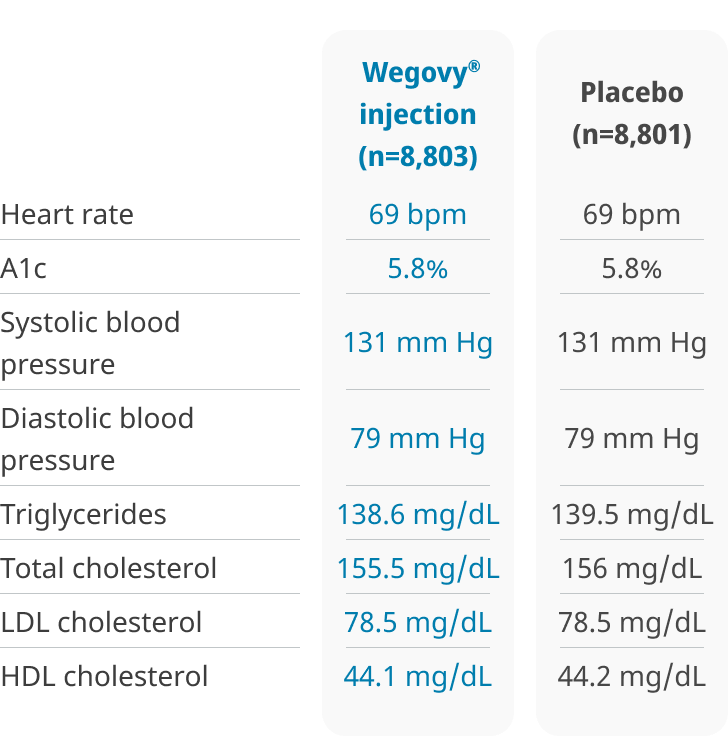
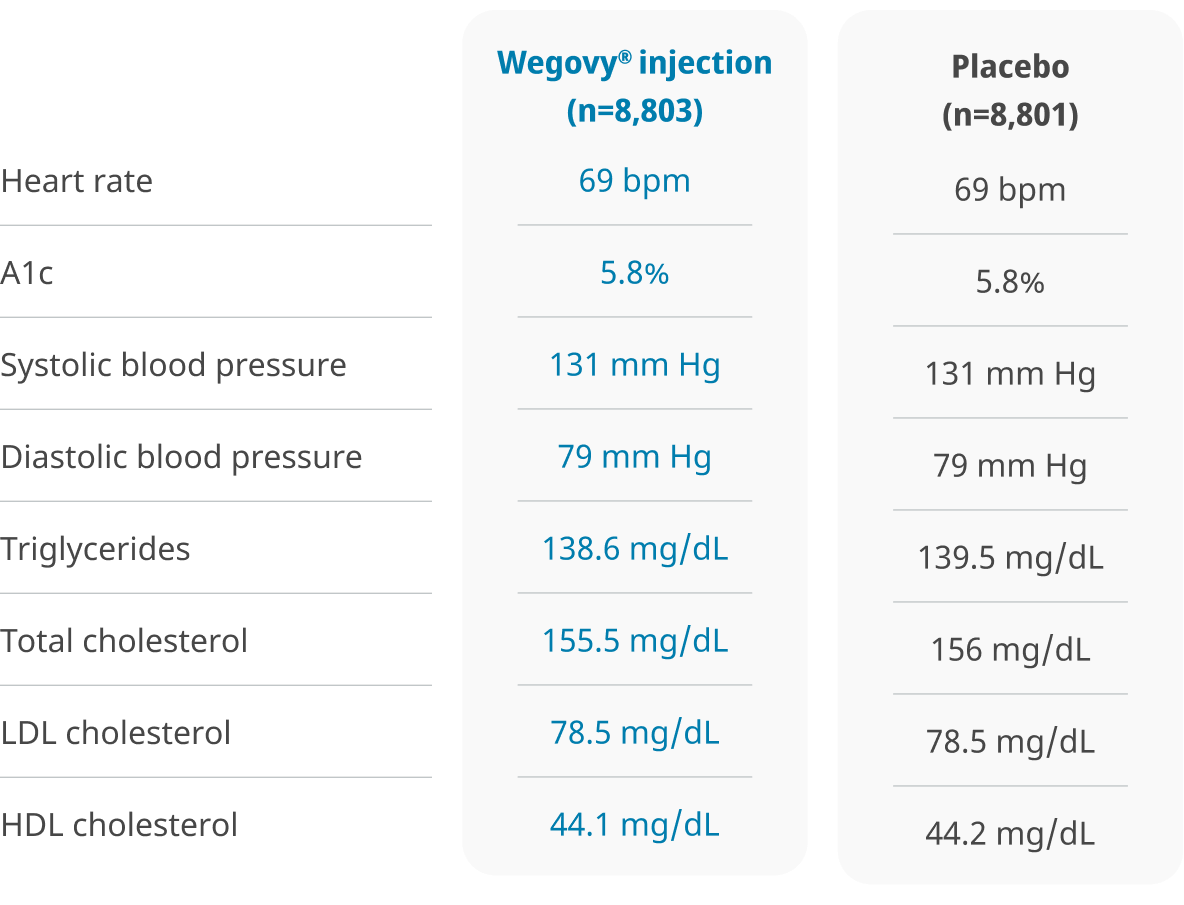
Heart rate
A1c
Systolic blood pressure
Diastolic blood pressure
Triglycerides
Total cholesterol
LDL cholesterol
HDL cholesterol
Wegovy® injection (n=8,803)
69 bpm
5.8%
131 mm Hg
79 mm Hg
138.6 mg/dL
155.5 mg/dL
78.5 mg/dL
44.1 mg/dL
Placebo
(n=8,801)
69 bpm
5.8%
131 mm Hg
79 mm Hg
139.5 mg/dL
156 mg/dL
78.5 mg/dL
44.2 mg/dL
*Standard of care included CV risk-factor management and individualized healthy lifestyle counseling (including diet and physical activity).
†Defined as having died or attended the final trial visit.
‡Not a comprehensive list.
BMI, body mass index; CV, cardiovascular; CVD, cardiovascular disease; CVOT, cardiovascular outcomes trial; MACE, major adverse cardiovascular events; Ml, myocardial infarction; PAD, peripheral arterial disease.
SELECT CVOT Study
SELECT: In adults with established CVD and either obesity or overweight, without diabetes, when added to CV standard of care,
Wegovy® is proven to help prevent life-threatening CV events1,2,4
Cardiovascular disease is the #1 cause of death for adults with obesity5
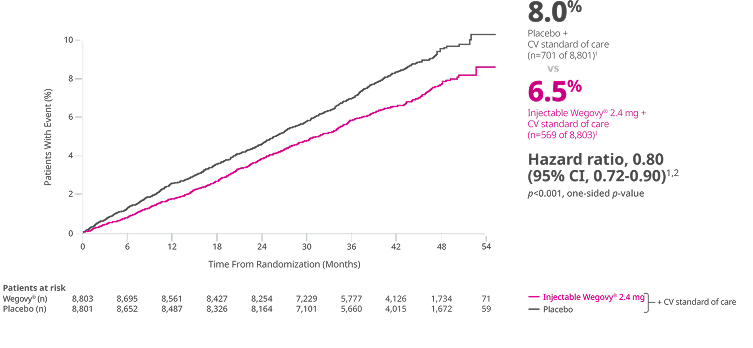
Primary composite end point: Time to first occurrence of MACE (CV death, non-fatal MI, or non-fatal stroke)1,2
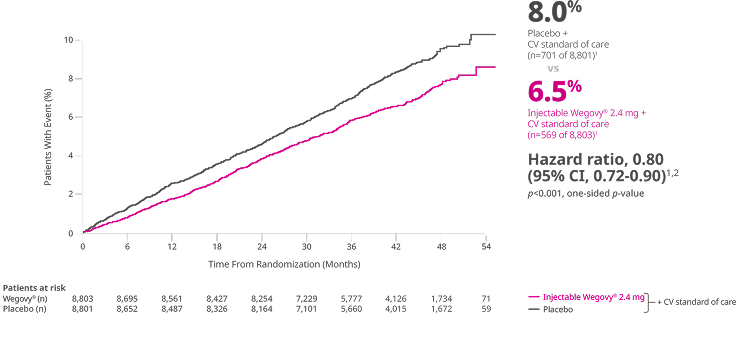
The exact mechanism of cardiovascular risk reduction of Wegovy® has not been established.1
The results from SELECT are based on a trial with injectable Wegovy® 2.4 mg


RRR of MACE
when added to CV SOC1,2
1.5% ARR3§
With Wegovy®, the reduction of MACE was not impacted by age, sex, race, ethnicity, BMI at baseline, or level of renal function impairment.1
SELECT1,2: Event-driven CVOT of 17,604 adults with obesity or overweight and established CVD (prior MI, prior stroke, or PAD) assessing superiority of once-weekly injectable Wegovy® 2.4 mg vs placebo (1:1 randomization) for time to first MACE. Both groups received standard of care for CV risk reduction. Patients with diabetes were excluded. Click to see full study design below.
§1.5% ARR at 40 months (mean duration of follow-up).3
ARR, absolute risk reduction; CI, confidence interval; RRR, relative risk reduction; SOC, standard of care.
You can prescribe appropriate patients looking for MACE risk reduction the Wegovy® pen or pill
Treatment effect for MACE and other events in SELECT1
The effects of semaglutide were directionally similar across end points1
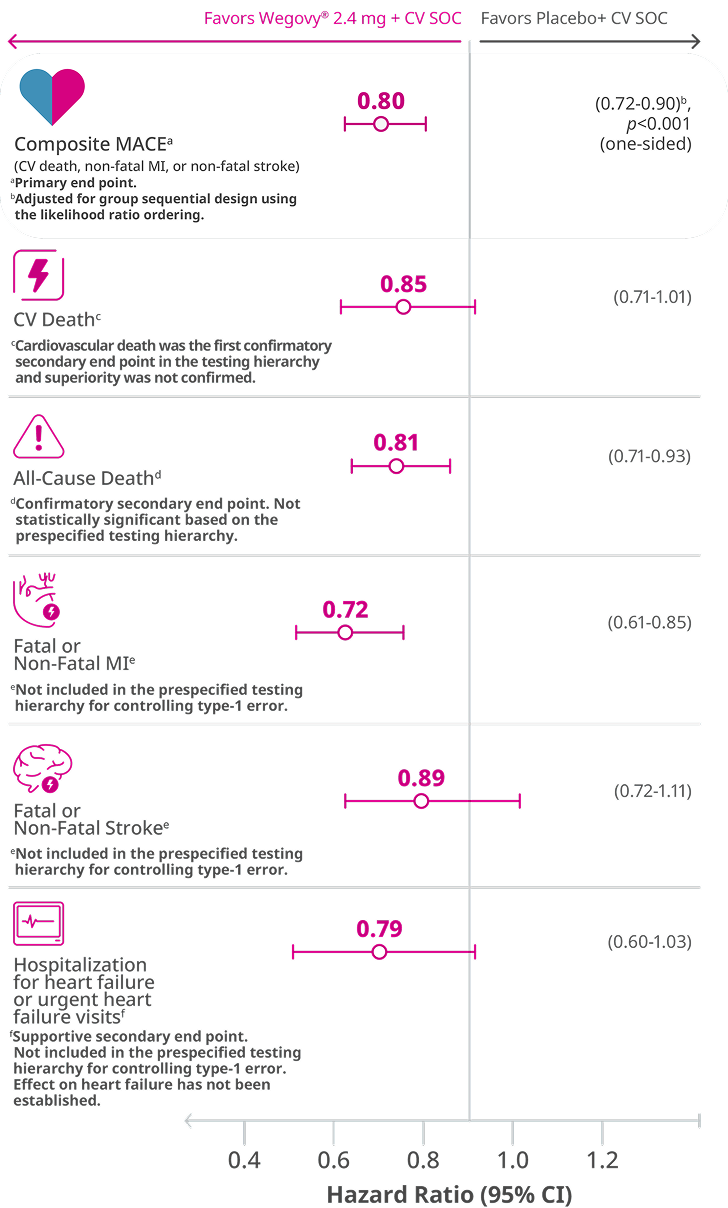
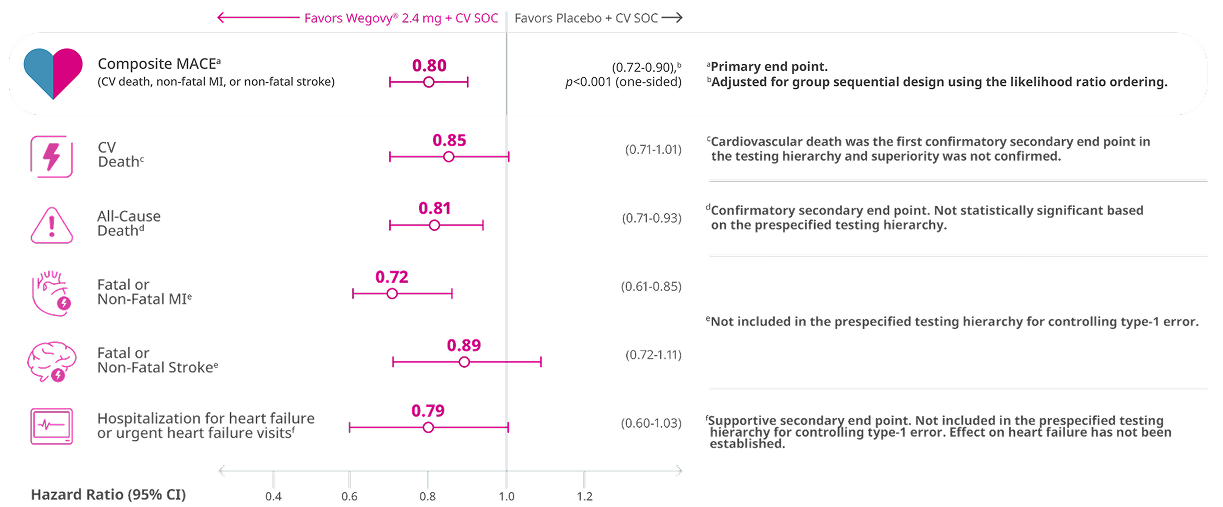
Wegovy® is not indicated to reduce the risk of heart failure events.
- CV death occurred in 2.5% (223/8,803) of patients on Wegovy® and 3.0% (262/8,801) of patients on placebo1
- All-cause death occurred in 4.3% (375/8,803) of patients on Wegovy® and 5.2% (458/8,801) of patients on placebo1
- Fatal or non-fatal MI occurred in 2.8% (243/8,803) of patients on Wegovy® and 3.8% (334/8,801) of patients on placebo1
- Fatal or non-fatal stroke occurred in 1.8% (160/8,803) of patients on Wegovy® and 2.0% (178/8,801) of patients on placebo1
- Hospitalization for heart failure or urgent heart failure visits occurred in 1.1% (97/8,803) of patients on Wegovy® and 1.4% (122/8,801) of patients on placebo1
SELECT CVOT Study
In the same study,
Patients taking Wegovy® experienced improvements across most cardiometabolic risk factors1
Supportive secondary end points: Change from baseline to week 104 in:
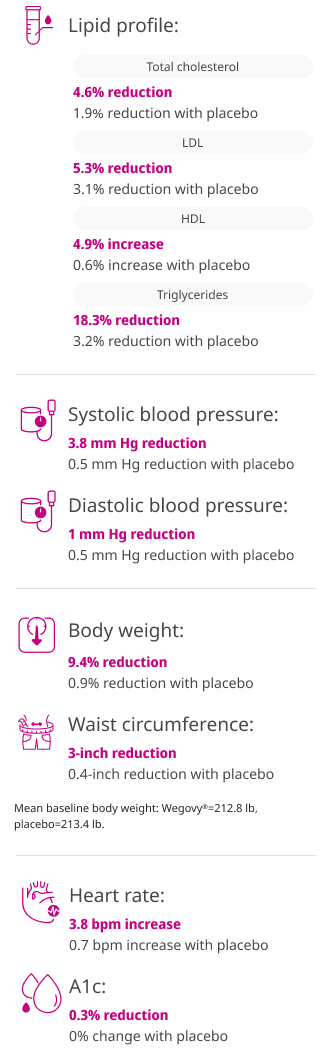
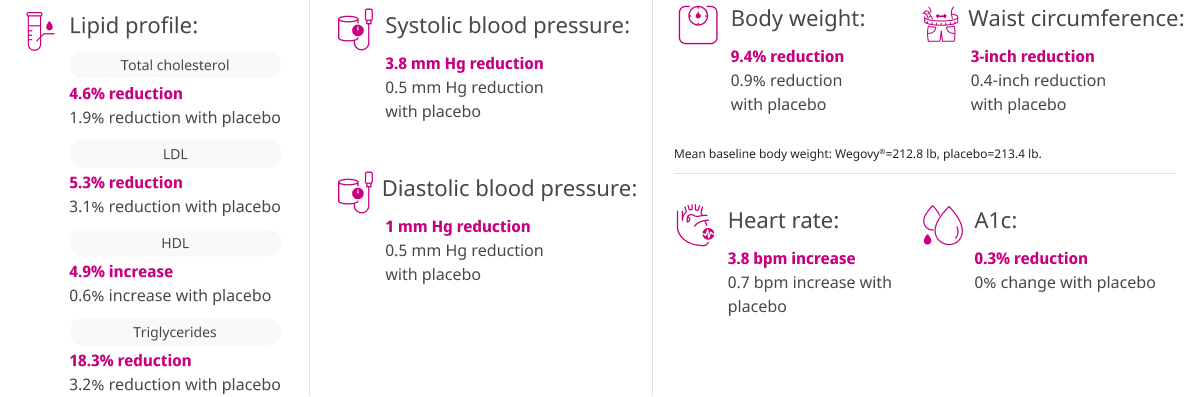
Wegovy® is not indicated to treat hypertension, type 2 diabetes, or dyslipidemia.
Supportive secondary end points were not included in the statistical testing hierarchy and, as such, not controlled for multiplicity.
A1c, glycated hemoglobin; bpm, beats per minute; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
SELECT Post Hoc Analysis
Early reduction in MACE was observed at 3 months with Wegovy® before clinically meaningful changes in body weight were seen3
Primary composite end point: Time to first occurrence of MACE (CV death, non-fatal MI, or non-fatal stroke)1,3
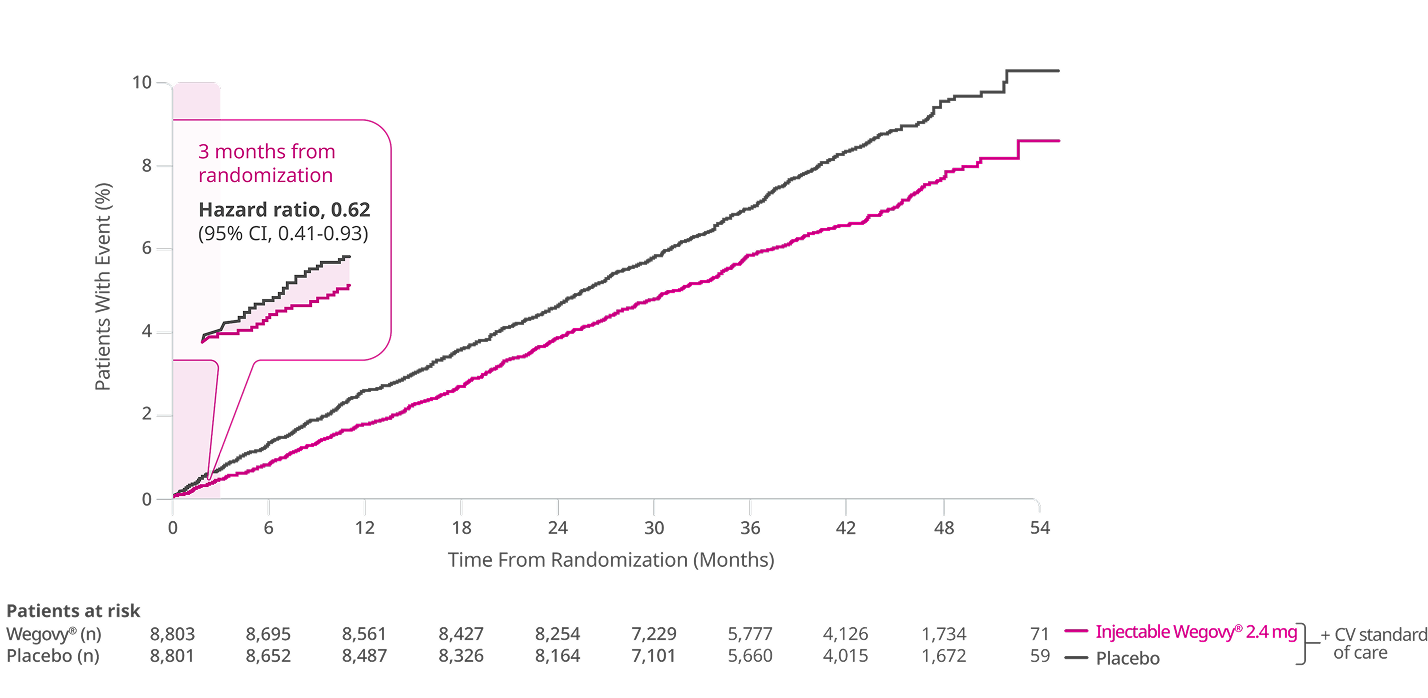
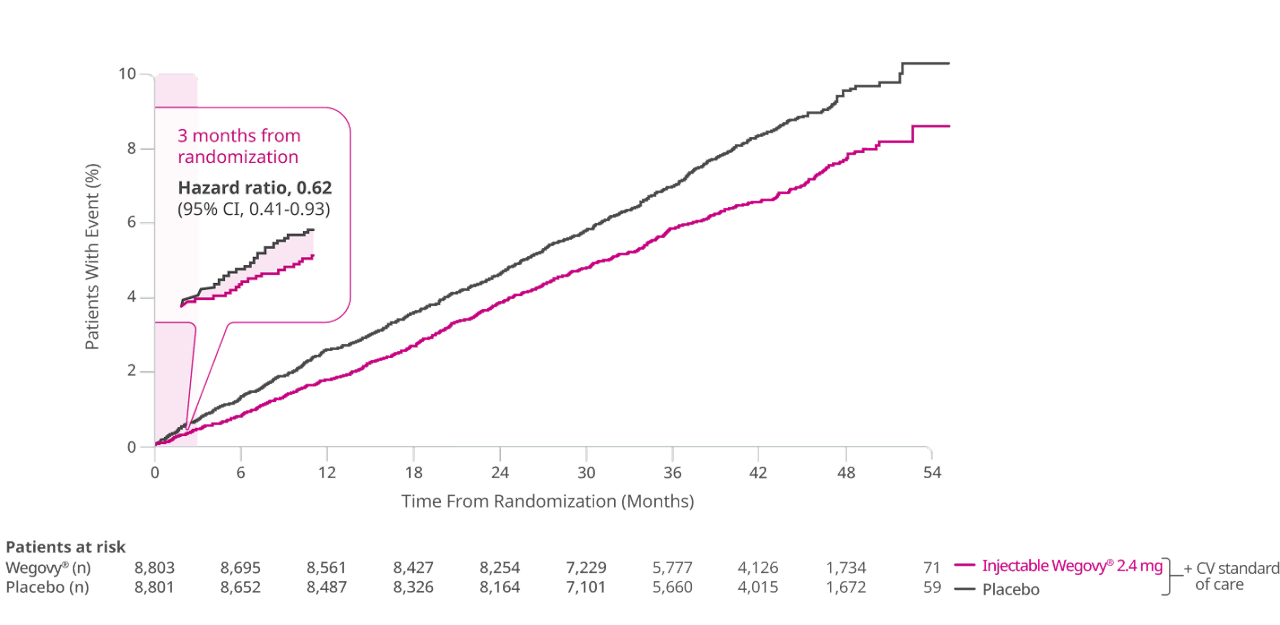
At week 12, estimated mean change in body weight from baseline was -4.1% in the Wegovy® arm and -0.6% in the placebo arm.3
Limitations:
- This post hoc analysis is hypothesis generating only; the clinical validity of these results cannot be determined
- SELECT was not powered for this analysis; Novo Nordisk was responsible for data analysis
- Further work addressing the mechanisms by which semaglutide produces these early clinical benefits would be of value3
Time to first MACE: Incidence over time3
Number of events
Month
Wegovy®
Placebo
0-3
36
58
The exact mechanism of cardiovascular risk reduction has not been established.1
Clinically meaningful weight loss is generally defined as ≥5% weight loss from baseline.6
Please click here for full SELECT study design.
SELECT CVOT Study
Please first review the SELECT data before assessing the SCORE real-world data.
Randomized clinical trials (RCTs)7,8
- Evaluate the safety and efficacy of a treatment in specific populations under controlled conditions
- Prospective designs with prespecified, well-defined inclusion/exclusion criteria, outcomes, and end points
- Patients are randomly assigned to treatment or comparator
Limitations:
- Tightly controlled conditions and inclusion/exclusion criteria of RCTs may limit generalizability to real-world conditions or clinical populations
- Can be expensive and time-consuming
Randomized clinical trials are designed to show causality7,8
Real-world evidence (RWE)8,9
- Use data from routine clinical practice
- Capture outcomes across broad patient populations
- Offer insight into how treatments perform outside of a controlled clinical trial setting
- Should be viewed as complementary to clinical trial data
Limitations:
- Susceptible to bias and confounding due to factors such as lack of randomization, missing or duplicative data, coding inaccuracies, and data variability reflecting routine clinical practice
Real-world studies evaluate associations and cannot determine causality8,9
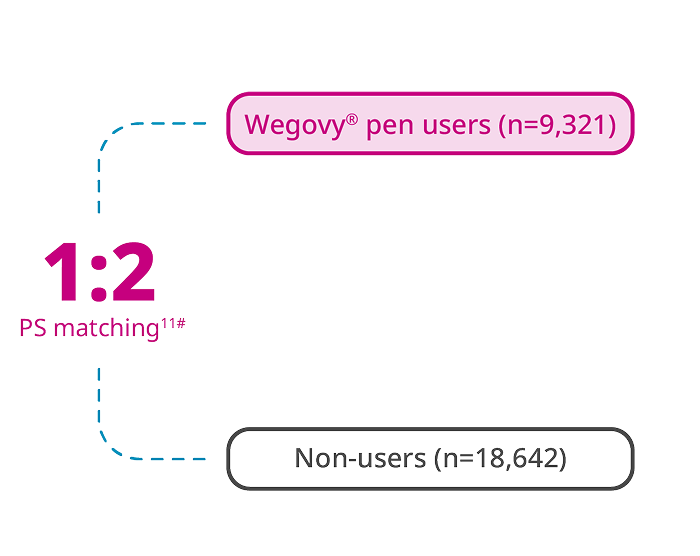
SCORE: The largest real-world CV outcomes study assessing the effectiveness of Wegovy® in adults with established CVD and overweight or obesity10 ‖
Patient population10
27,963
patients
Baseline period: 12 months prior to index date11
Key Inclusion Criteria10¶
Adults: ≥45 years
Overweight or obesity
(BMI: ≥27 kg/m2)
Established CVD:
• Prior MI
• Ischemic stroke
• PAD
No prior history of diabetes

Treatment arms10

End point assessed10
MACE-3
CV Death** Non-Fatal MI Non-Fatal Stroke
Patients were followed until the
earliest instance of10:
• The earliest instance of the end of continuous enrollment or of data availability
• The initiation of a (non-semaglutide) GLP-1 or GLP-1/GIP receptor agonist
• A bariatric surgical procedure
• Death
This study used the Komodo research database, which includes administrative medical and pharmacy claims linked with clinical and laboratory measurements for patients in the US during January 1, 2016-December 31, 2023.
Index date definition: Wegovy® injection users: The initiation date of Wegovy® in a pharmacy claim on or after June 4, 2021. Non-users: A randomly selected date with 21 pharmacy claim(s) on or after June 4, 2021.
Patients were followed until the earliest instance of the end of continuous enrollment or of data availability, initiation of a (non-semaglutide) GLP-1 or GIP/GLP-1 receptor agonist, bariatric surgical procedure, or death.
∥As of March 24, 2025.
¶Inclusion criteria and end points were identified by ICD-10 codes, procedural codes, or recorded measurements (BMI).
#A non-parsimonious PS model was used to alleviate the effect of potential confounding on systematic differences in patient characteristics based on treatment exposure. Over 50 variables were matched, including: age, gender, race/ethnicity, region, insurance type, index year, duration between the eligibility date and index date, BMI, smoking history, comorbidities, procedures, medication use, and health care resource utilization.
**CV death: Death within ≤30 days of a CV event.
GIP, glucose-dependent insulinotropic polypeptide; GLP-1, glucagon-like peptide-1; PS, propensity score.
Incidence of MACE with Wegovy® in a real-world study
Outcome: Time to first occurrence of MACE-3 (CV death, non-fatal MI, non-fatal stroke)10
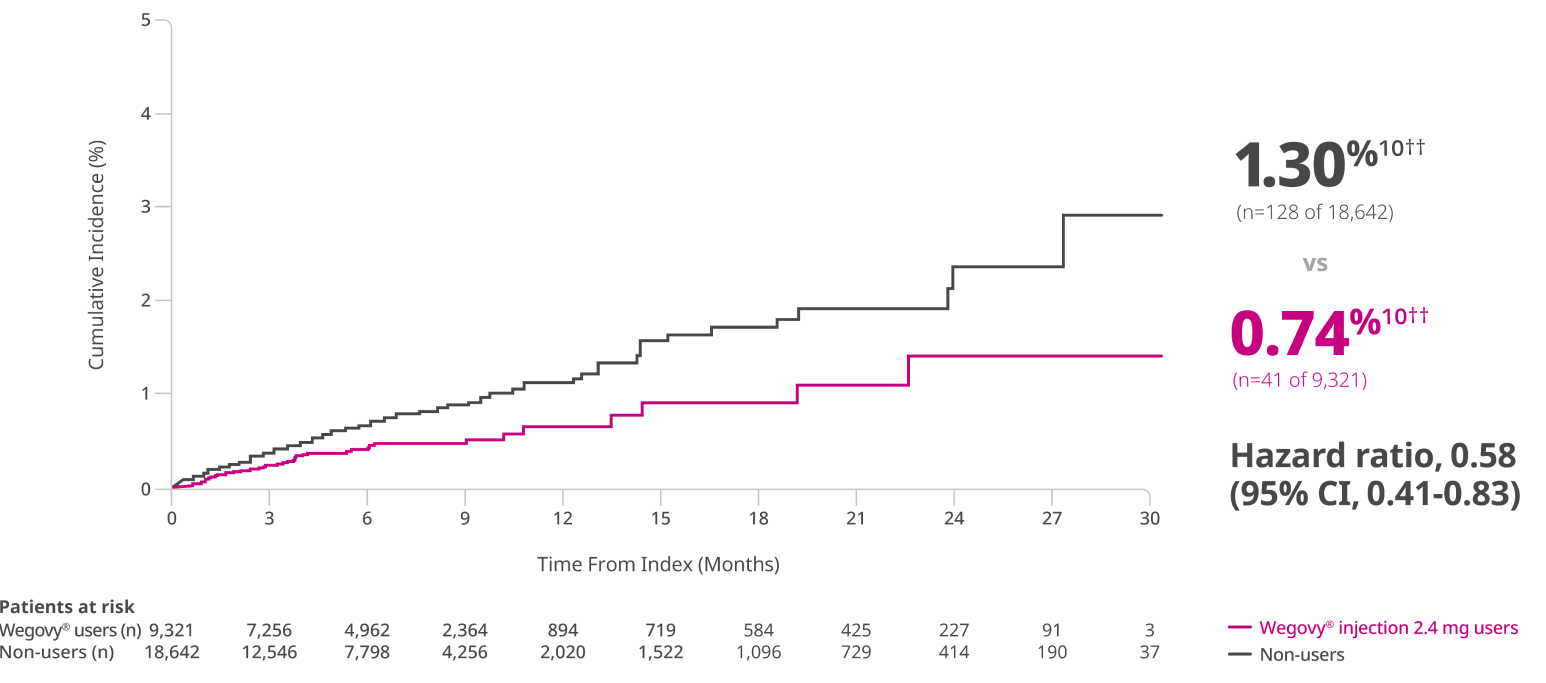
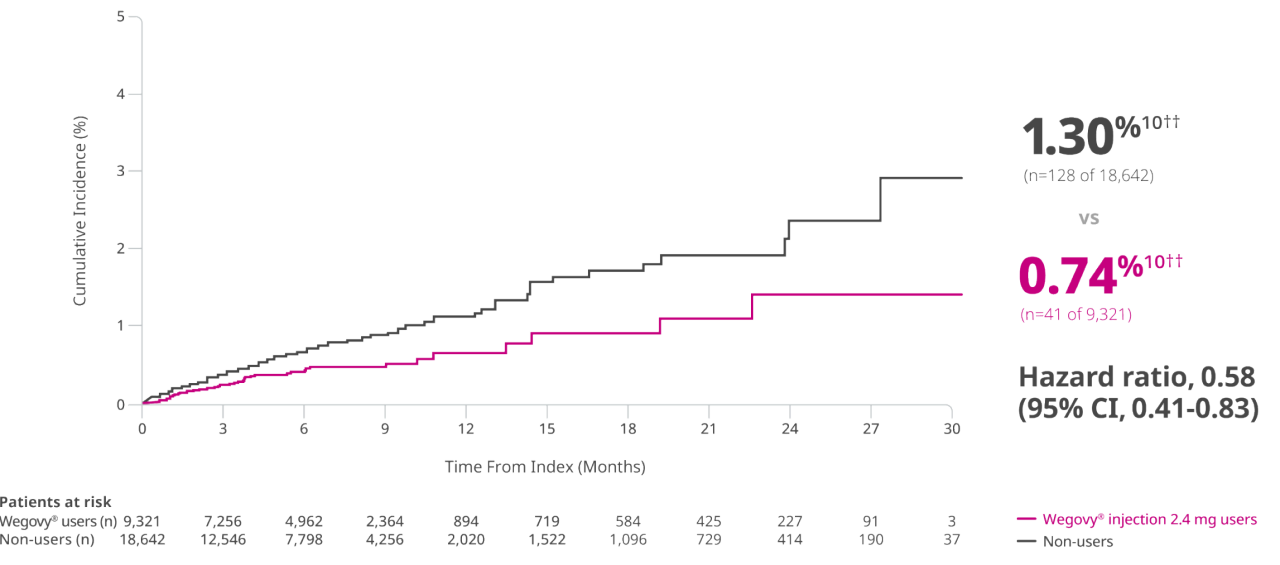
Results should be interpreted in the context of the limitations of this study.
In Wegovy® pen users vs non-users3,10
Mean duration of follow-up: 7.1 months
with Wegovy® users; 6.4 months with
non-users
Limitations: Despite robust PS matching and multiple sensitivity analyses, the potential for residual unmeasured confounding exists. The approval of Wegovy® in 2021 resulted in a relatively short duration of follow-up, limiting assessment of long-term outcomes. Requiring 12 months of continuous coverage before the index date may exclude patients with intermittent insurance coverage or those from underserved populations, limiting generalizability.10
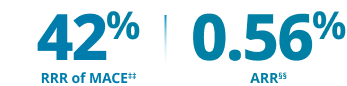
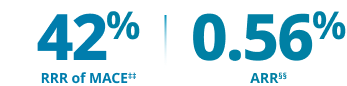
††Event rates per person-year: 41 events over 5,519 person-years for Wegovy® injection users, 128 events over 9,859 person-years for non-users.
‡‡The relative risk reduction is approximated by 1-hazard ratio.
§§ARR represents the difference in event rates per person-year in semaglutide users vs non-users.
Study designs
SELECT1,2: A multi-national, double-blind, placebo-controlled, event-driven CV outcomes trial of 17,604 adults with a BMI ≥27 kg/m2 and established CVD (prior MI, prior stroke, or PAD) assessing superiority of once-weekly injectable Wegovy® 2.4 mg vs placebo (1:1 randomization, with a 16-week dose escalation) for time to first MACE. Both groups received current standard of care, including CV risk factor management and individualized healthy lifestyle counseling (including diet and physical activity); concomitant CV therapies could be adjusted, at the discretion of the investigator, to ensure participants were treated according to the current standard of care for patients with established CVD. Patients with a history of type 1 or type 2 diabetes were excluded. Median duration of follow-up was 41.8 months.
Primary composite end point2:
- Time from randomization to first occurrence of a 3-part composite MACE, defined as CV death, non-fatal MI, or non-fatal stroke
Key secondary end points2:
Time from randomization to first occurrence of:
- Cardiovascular death
- All-cause death
Other secondary end points2:
Time from randomization to first occurrence of:
- Fatal or non-fatal myocardial infarction
- Fatal or non-fatal stroke
Relevant supportive secondary end points2:
- Change in body weight from baseline to week 104
- Change in waist circumference from baseline to week 104
- Change in systolic blood pressure from baseline to week 104
- Change in diastolic blood pressure from baseline to week 104
- Change in heart rate from baseline to week 104
- Change in A1c from baseline to week 104
- Change in lipids∥∥ from baseline to week 104
∥∥LDL, HDL, triglycerides, and total cholesterol.
SCORE3,10: A retrospective observational study using the Komodo Research Dataset (EHR linked to medical and pharmacy claims) of 27,963 US adults with a BMI ≥27 kg/m2 and established CVD (prior MI, prior stroke, or PAD) comparing the incidence of MACE-3 (CV death, non-fatal MI, or non-fatal stroke) in Wegovy® injection users vs non-users without diabetes. Full study period was from January 1, 2016, to December 31, 2023. Index date was defined as first Wegovy® claim or randomly selected pharmacy claim on or after June 4, 2021, for Wegovy® injection users and non-users, respectively. Baseline period was 12 months prior to the index date. Wegovy® injection users and non-users were matched using a non-parsimonious PS model to alleviate the effect of potential confounding on systematic differences in patient characteristics. Over 50 variables were matched, including age, gender, race/ethnicity, region, insurance type, index year, duration between the eligibility date and index date, BMI, smoking history, comorbidities, procedures, medication use, and health care resource utilization.
End point:
- Time to first occurrence of MACE-3 (CV death, non-fatal MI, or non-fatal stroke)
EHR, electronic health record.
SELECT CVOT Study
Wegovy® can help your patients who have had a prior CV event1
Added to CV standard of care therapy, Wegovy® can help manage CV risk for patients living with cardiovascular disease and obesity or overweight
Henry
AGED 68 YEARS
CV History
Previous MI (>5 years ago)
BMI
29.5 kg/m2
Current Treatments Include
Statin and beta-blocker
Comorbidities and History
Hyperlipidemia, hypertension, no type 2 diabetes
Insurance Coverage
Medicare

Robert
AGED 65 YEARS
CV History
Recent stroke (4 months ago)
BMI
41 kg/m2
Current Treatments Include
Oral anticoagulant
Comorbidities and History
No type 2 diabetes, history of smoking
Insurance Coverage
Medicare

Brenda
AGED 59 YEARS
CV History
Recent MI (5 months ago)
BMI
31 kg/m2
Current Treatments Include
Platelet aggregation inhibitor
Comorbidities and History
No type 2 diabetes
Insurance Coverage
Commercial

Actor portrayals. Hypothetical patients for demonstrative purposes only.
Verify your patient’s Wegovy® coverage
See long-term weight-management results
Important Safety Information for Wegovy®
WARNING: RISK OF THYROID C-CELL TUMORS
- In rodents, semaglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures. It is unknown whether Wegovy® causes thyroid C-cell tumors, including medullary thyroid carcinoma (MTC), in humans as human relevance of semaglutide-induced rodent thyroid C-cell tumors has not been determined
- Wegovy® is contraindicated in patients with a personal or family history of MTC or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). Counsel patients regarding the potential risk for MTC with the use of Wegovy® and inform them of symptoms of thyroid tumors (e.g. a mass in the neck, dysphagia, dyspnea, persistent hoarseness). Routine monitoring of serum calcitonin or using thyroid ultrasound is of uncertain value for early detection of MTC in patients treated with Wegovy®
Contraindications
- Wegovy® is contraindicated in patients with a personal or family history of MTC or in patients with MEN 2, and in patients with a prior serious hypersensitivity reaction to semaglutide or to any of the excipients in Wegovy®. Serious hypersensitivity reactions, including anaphylaxis and angioedema have been reported with Wegovy®
Warnings and Precautions
- Risk of Thyroid C-Cell Tumors: Patients should be further evaluated if serum calcitonin is measured and found to be elevated or thyroid nodules are noted on physical examination or neck imaging
- Acute Pancreatitis: Acute pancreatitis, including fatal and non-fatal hemorrhagic or necrotizing pancreatitis, has been observed in patients treated with GLP-1 receptor agonists, including Wegovy®. Observe patients carefully for signs and symptoms of acute pancreatitis, which may include persistent or severe abdominal pain (sometimes radiating to the back), and which may or may not be accompanied by nausea, or vomiting. If pancreatitis is suspected, discontinue Wegovy® and initiate appropriate management
- Acute Gallbladder Disease: Treatment with Wegovy® is associated with an increased occurrence of cholelithiasis and cholecystitis. The incidence of cholelithiasis and cholecystitis was higher in Wegovy® injection-treated pediatric patients aged ≥12 years than in Wegovy® injection-treated adults. In clinical trials in adult patients, cholelithiasis was reported by 1.6% of Wegovy® injection-treated patients and 0.7% of placebo treated patients, and by 2.5% of Wegovy® tablet-treated patients and 1% of placebo treated patients. Cholecystitis was reported by 0.6% of Wegovy® injection-treated adult patients and 0.2% of placebo treated patients. In a clinical trial in pediatric patients aged ≥12 years, cholelithiasis was reported by 3.8% of Wegovy® injection-treated patients and 0% placebo treated patients. Cholecystitis was reported by 0.8% of Wegovy® injection-treated pediatric patients and 0% placebo treated patients. Substantial or rapid weight loss can increase the risk of cholelithiasis; however, the incidence of acute gallbladder disease was greater in Wegovy® patients than in placebo patients, even after accounting for the degree of weight loss. If cholelithiasis is suspected, gallbladder studies and appropriate clinical follow-up are indicated
- Hypoglycemia: Wegovy® lowers blood glucose and can cause hypoglycemia. In a trial of Wegovy® injection in adult patients with type 2 diabetes (T2D) and a BMI ≥27 kg/m2, hypoglycemia was reported in more patients treated with Wegovy® versus placebo. In glycemic control clinical trials, the risk of hypoglycemia was increased when semaglutide injection or tablet was used concomitantly with insulin or an insulin secretagogue (e.g., sulfonylurea). Patients with diabetes taking Wegovy® with an insulin or insulin secretagogue may have an increased risk of hypoglycemia, including severe hypoglycemia. The use of Wegovy® in patients with type 1 diabetes or in combination with insulin has not been evaluated. Inform patients of the risk of hypoglycemia and educate them on the signs and symptoms. Monitor blood glucose in patients with diabetes
- Acute Kidney Injury Due to Volume Depletion: There have been postmarketing reports of acute kidney injury, in some cases requiring hemodialysis, in patients treated with semaglutide. The majority of the reported events occurred in patients who experienced gastrointestinal reactions leading to dehydration such as nausea, vomiting, or diarrhea. Monitor renal function in patients reporting adverse reactions to Wegovy® that could lead to volume depletion, especially during initiation and escalation of Wegovy®
- Severe Gastrointestinal (GI) Adverse Reactions: Use of Wegovy® has been associated with GI adverse reactions, sometimes severe. In adult clinical trials, severe GI adverse reactions were reported more frequently among patients receiving Wegovy® than placebo. Severe GI adverse reactions were reported in 4.1% and 0.9% of Wegovy®-injection treated and placebo treated patients, respectively, and in 2% of Wegovy® tablet-treated and 0% of placebo treated patients, respectively. Severe GI adverse reactions have also been reported postmarketing with GLP-1 receptor agonists. Wegovy® is not recommended in patients with severe gastroparesis
- Hypersensitivity Reactions: Serious hypersensitivity reactions (e.g., anaphylaxis, angioedema) have been reported with Wegovy®. If hypersensitivity reactions occur, discontinue use of Wegovy®, treat promptly per standard of care, and monitor until signs and symptoms resolve. Use caution in a patient with a history of anaphylaxis or angioedema with another GLP-1 receptor agonist
- Diabetic Retinopathy Complications in Patients with T2D: In a trial of adult patients with T2D and BMI ≥27 kg/m2, diabetic retinopathy was reported by 4% of Wegovy® injection-treated patients and 2.7% of placebo patients. In a glycemic control trial evaluating a dose comparable to the 9 mg dose and the 25 mg semaglutide tablet doses in patients with T2D, 1.3% and 1.9% of patients in the 9 mg and 25 mg semaglutide group, respectively, reported moderate-severe non-proliferative diabetic retinopathy events, and 0% and 0.4% reported proliferative retinopathy events, respectively. Rapid improvement in glucose control has been associated with a temporary worsening of diabetic retinopathy. Patients with a history of diabetic retinopathy should be monitored for progression of diabetic retinopathy
- Heart Rate Increase: Mean increases in resting heart rate of 1 to 4 beats per minute (bpm) were observed in Wegovy® injection-treated adult patients compared to placebo in clinical trials. More adults treated with Wegovy® injection compared with placebo had maximum changes from baseline of 10 to 19 bpm (41% vs 34%) and 20 bpm or more (26% vs 16%). In a clinical trial in pediatric patients aged ≥12 years with normal baseline heart rate, more patients treated with Wegovy® injection compared to placebo had maximum changes in heart rate of 20 bpm or more (54% vs 39%). Findings were similar in a trial with the Wegovy® tablets. Monitor heart rate at regular intervals and instruct patients to report palpitations or feelings of a racing heartbeat while at rest. If patients experience a sustained increase in resting heart rate, discontinue Wegovy®
- Pulmonary Aspiration During General Anesthesia or Deep Sedation: Wegovy® delays gastric emptying. There have been rare postmarketing reports of pulmonary aspiration in patients receiving GLP-1 receptor agonists undergoing elective surgeries or procedures requiring general anesthesia or deep sedation who had residual gastric contents despite reported adherence to preoperative fasting recommendations. Instruct patients to inform healthcare providers prior to any planned surgeries or procedures if they are taking Wegovy®
- Never Share Wegovy® FlexTouch® Between Patients: Wegovy® FlexTouch® must never be shared between patients, even if the needle is changed. Pen-sharing poses a risk for transmission of blood-borne pathogens
Adverse Reactions
- Most common adverse reactions (incidence ≥5%) are: nausea, diarrhea, vomiting, constipation, abdominal pain, dysesthesia, headache, fatigue, dyspepsia, dizziness, abdominal distention, eructation, hypoglycemia in patients with T2D, flatulence, gastroenteritis, gastroesophageal reflux disease, and hair loss
Drug Interactions
- When initiating Wegovy®, consider reducing the dose of concomitantly administered insulin secretagogues or insulin to reduce the risk of hypoglycemia. The addition of Wegovy® in patients treated with insulin has not been evaluated
- Wegovy® causes a delay of gastric emptying and has the potential to impact the absorption of concomitantly administered oral medications. Monitor the effects of oral medications concomitantly administered with Wegovy®. Consider increased clinical or laboratory monitoring for medications that have a narrow therapeutic index or that require clinical monitoring
Use in Specific Populations
- Pregnancy: May cause fetal harm. When pregnancy is recognized, advise the pregnant patient of the risk to a fetus. Discontinue Wegovy® in pregnant patients who are using Wegovy® for weight reduction or at least 2 months before a planned pregnancy
- Lactation: A clinical lactation study reported semaglutide concentrations below the lower limit of quantification in human breast milk. However, salcaprozate sodium (SNAC) and/or its metabolites are present in human milk. Because of the unknown potential for serious adverse reactions in the breastfed infant due to the possible accumulation of SNAC, an absorption enhancer for Wegovy® tablets, and because there are alternative formulations of semaglutide that do not contain SNAC that can be used during lactation, advise patients that breastfeeding is not recommended during treatment with Wegovy® tablets
- Pediatric: Adverse reactions with Wegovy® injection-treated pediatric patients ≥12 years with obesity were similar to those reported in adults. Pediatric patients ≥12 years treated with Wegovy® injection had greater incidences of cholelithiasis, cholecystitis, hypotension, rash, and urticaria compared to adults treated with Wegovy®. There are insufficient data in pediatric patients with T2D treated with Wegovy® injection for obesity to determine if there is an increased risk of hypoglycemia with Wegovy® injection treatment similar to that reported in adults.
The safety and effectiveness of Wegovy® injection have not been established in pediatric patients to reduce the risk of major adverse CV events or to reduce excess body weight and maintain weight reduction long term with the 7.2 mg once weekly dosage or in those <12 years.
The safety and effectiveness of Wegovy® tablets have not been established in pediatric patients - Geriatric: In the CV outcomes trial, patients ≥75 years reported more hip and pelvis fractures on Wegovy® injection than placebo. Patients ≥75 years (Wegovy® injection and placebo) reported more serious adverse reactions overall compared to younger adult patients
- Type 2 Diabetes: Wegovy® tablets have not been studied for weight reduction in adults with T2D and obesity or overweight. Administration of Wegovy® injection resulted in less weight reduction in patients with T2D and obesity or overweight compared to those without T2D and obesity or overweight
Please click here for Wegovy® Prescribing Information, including Boxed Warning.
Indications and Usage
Wegovy® (semaglutide) injection is indicated in combination with a reduced calorie diet and increased physical activity:
- To reduce the risk of major adverse cardiovascular (CV) events (CV death, non-fatal myocardial infarction, or non-fatal stroke) in adults with established CV disease and either obesity or overweight
- To reduce excess body weight and maintain weight reduction long term in:
- Adults and pediatric patients 12 years and older with obesity
- Adults with overweight in the presence of at least one weight-related comorbidity
Wegovy® (semaglutide) tablets are indicated in combination with a reduced calorie diet and increased physical activity to:
- Reduce the risk of major adverse cardiovascular (CV) events (CV death, non-fatal myocardial infarction, or non-fatal stroke) in adults with established CV disease and either obesity or overweight
- Reduce excess body weight and maintain weight reduction long term in adults with obesity or with overweight in the presence of at least one weight-related comorbidity
Limitations of Use:
Concomitant use of Wegovy® tablets or Wegovy® injection with other semaglutide-containing products or with any GLP-1 receptor agonist is not recommended
Important Safety Information for Wegovy®
WARNING: RISK OF THYROID C-CELL TUMORS
- In rodents, semaglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures. It is unknown whether Wegovy® causes thyroid C-cell tumors, including medullary thyroid carcinoma (MTC), in humans as human relevance of semaglutide-induced rodent thyroid C-cell tumors has not been determined
- Wegovy® is contraindicated in patients with a personal or family history of MTC or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). Counsel patients regarding the potential risk for MTC with the use of Wegovy® and inform them of symptoms of thyroid tumors (e.g. a mass in the neck, dysphagia, dyspnea, persistent hoarseness). Routine monitoring of serum calcitonin or using thyroid ultrasound is of uncertain value for early detection of MTC in patients treated with Wegovy®
Important Safety Information for Wegovy®
WARNING: RISK OF THYROID C-CELL TUMORS
- In rodents, semaglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures. It is unknown whether Wegovy® causes thyroid C-cell tumors, including medullary thyroid carcinoma (MTC), in humans as human relevance of semaglutide-induced rodent thyroid C-cell tumors has not been determined
- Wegovy® is contraindicated in patients with a personal or family history of MTC or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). Counsel patients regarding the potential risk for MTC with the use of Wegovy® and inform them of symptoms of thyroid tumors (e.g. a mass in the neck, dysphagia, dyspnea, persistent hoarseness). Routine monitoring of serum calcitonin or using thyroid ultrasound is of uncertain value for early detection of MTC in patients treated with Wegovy®
Contraindications
- Wegovy® is contraindicated in patients with a personal or family history of MTC or in patients with MEN 2, and in patients with a prior serious hypersensitivity reaction to semaglutide or to any of the excipients in Wegovy®. Serious hypersensitivity reactions, including anaphylaxis and angioedema have been reported with Wegovy®
Warnings and Precautions
- Risk of Thyroid C-Cell Tumors: Patients should be further evaluated if serum calcitonin is measured and found to be elevated or thyroid nodules are noted on physical examination or neck imaging
- Acute Pancreatitis: Acute pancreatitis, including fatal and non-fatal hemorrhagic or necrotizing pancreatitis, has been observed in patients treated with GLP-1 receptor agonists, including Wegovy®. Observe patients carefully for signs and symptoms of acute pancreatitis, which may include persistent or severe abdominal pain (sometimes radiating to the back), and which may or may not be accompanied by nausea, or vomiting. If pancreatitis is suspected, discontinue Wegovy® and initiate appropriate management
- Acute Gallbladder Disease: Treatment with Wegovy® is associated with an increased occurrence of cholelithiasis and cholecystitis. The incidence of cholelithiasis and cholecystitis was higher in Wegovy® injection-treated pediatric patients aged ≥12 years than in Wegovy® injection-treated adults. In clinical trials in adult patients, cholelithiasis was reported by 1.6% of Wegovy® injection-treated patients and 0.7% of placebo treated patients, and by 2.5% of Wegovy® tablet-treated patients and 1% of placebo treated patients. Cholecystitis was reported by 0.6% of Wegovy® injection-treated adult patients and 0.2% of placebo treated patients. In a clinical trial in pediatric patients aged ≥12 years, cholelithiasis was reported by 3.8% of Wegovy® injection-treated patients and 0% placebo treated patients. Cholecystitis was reported by 0.8% of Wegovy® injection-treated pediatric patients and 0% placebo treated patients. Substantial or rapid weight loss can increase the risk of cholelithiasis; however, the incidence of acute gallbladder disease was greater in Wegovy® patients than in placebo patients, even after accounting for the degree of weight loss. If cholelithiasis is suspected, gallbladder studies and appropriate clinical follow-up are indicated
- Hypoglycemia: Wegovy® lowers blood glucose and can cause hypoglycemia. In a trial of Wegovy® injection in adult patients with type 2 diabetes (T2D) and a BMI ≥27 kg/m2, hypoglycemia was reported in more patients treated with Wegovy® versus placebo. In glycemic control clinical trials, the risk of hypoglycemia was increased when semaglutide injection or tablet was used concomitantly with insulin or an insulin secretagogue (e.g., sulfonylurea). Patients with diabetes taking Wegovy® with an insulin or insulin secretagogue may have an increased risk of hypoglycemia, including severe hypoglycemia. The use of Wegovy® in patients with type 1 diabetes or in combination with insulin has not been evaluated. Inform patients of the risk of hypoglycemia and educate them on the signs and symptoms. Monitor blood glucose in patients with diabetes
- Acute Kidney Injury Due to Volume Depletion: There have been postmarketing reports of acute kidney injury, in some cases requiring hemodialysis, in patients treated with semaglutide. The majority of the reported events occurred in patients who experienced gastrointestinal reactions leading to dehydration such as nausea, vomiting, or diarrhea. Monitor renal function in patients reporting adverse reactions to Wegovy® that could lead to volume depletion, especially during initiation and escalation of Wegovy®
- Severe Gastrointestinal (GI) Adverse Reactions: Use of Wegovy® has been associated with GI adverse reactions, sometimes severe. In adult clinical trials, severe GI adverse reactions were reported more frequently among patients receiving Wegovy® than placebo. Severe GI adverse reactions were reported in 4.1% and 0.9% of Wegovy®-injection treated and placebo treated patients, respectively, and in 2% of Wegovy® tablet-treated and 0% of placebo treated patients, respectively. Severe GI adverse reactions have also been reported postmarketing with GLP-1 receptor agonists. Wegovy® is not recommended in patients with severe gastroparesis
- Hypersensitivity Reactions: Serious hypersensitivity reactions (e.g., anaphylaxis, angioedema) have been reported with Wegovy®. If hypersensitivity reactions occur, discontinue use of Wegovy®, treat promptly per standard of care, and monitor until signs and symptoms resolve. Use caution in a patient with a history of anaphylaxis or angioedema with another GLP-1 receptor agonist
- Diabetic Retinopathy Complications in Patients with T2D: In a trial of adult patients with T2D and BMI ≥27 kg/m2, diabetic retinopathy was reported by 4% of Wegovy® injection-treated patients and 2.7% of placebo patients. In a glycemic control trial evaluating a dose comparable to the 9 mg dose and the 25 mg semaglutide tablet doses in patients with T2D, 1.3% and 1.9% of patients in the 9 mg and 25 mg semaglutide group, respectively, reported moderate-severe non-proliferative diabetic retinopathy events, and 0% and 0.4% reported proliferative retinopathy events, respectively. Rapid improvement in glucose control has been associated with a temporary worsening of diabetic retinopathy. Patients with a history of diabetic retinopathy should be monitored for progression of diabetic retinopathy
- Heart Rate Increase: Mean increases in resting heart rate of 1 to 4 beats per minute (bpm) were observed in Wegovy® injection-treated adult patients compared to placebo in clinical trials. More adults treated with Wegovy® injection compared with placebo had maximum changes from baseline of 10 to 19 bpm (41% vs 34%) and 20 bpm or more (26% vs 16%). In a clinical trial in pediatric patients aged ≥12 years with normal baseline heart rate, more patients treated with Wegovy® injection compared to placebo had maximum changes in heart rate of 20 bpm or more (54% vs 39%). Findings were similar in a trial with the Wegovy® tablets. Monitor heart rate at regular intervals and instruct patients to report palpitations or feelings of a racing heartbeat while at rest. If patients experience a sustained increase in resting heart rate, discontinue Wegovy®
- Pulmonary Aspiration During General Anesthesia or Deep Sedation: Wegovy® delays gastric emptying. There have been rare postmarketing reports of pulmonary aspiration in patients receiving GLP-1 receptor agonists undergoing elective surgeries or procedures requiring general anesthesia or deep sedation who had residual gastric contents despite reported adherence to preoperative fasting recommendations. Instruct patients to inform healthcare providers prior to any planned surgeries or procedures if they are taking Wegovy®
- Never Share Wegovy® FlexTouch® Between Patients: Wegovy® FlexTouch® must never be shared between patients, even if the needle is changed. Pen-sharing poses a risk for transmission of blood-borne pathogens
Adverse Reactions
- Most common adverse reactions (incidence ≥5%) are: nausea, diarrhea, vomiting, constipation, abdominal pain, dysesthesia, headache, fatigue, dyspepsia, dizziness, abdominal distention, eructation, hypoglycemia in patients with T2D, flatulence, gastroenteritis, gastroesophageal reflux disease, and hair loss
Drug Interactions
- When initiating Wegovy®, consider reducing the dose of concomitantly administered insulin secretagogues or insulin to reduce the risk of hypoglycemia. The addition of Wegovy® in patients treated with insulin has not been evaluated
- Wegovy® causes a delay of gastric emptying and has the potential to impact the absorption of concomitantly administered oral medications. Monitor the effects of oral medications concomitantly administered with Wegovy®. Consider increased clinical or laboratory monitoring for medications that have a narrow therapeutic index or that require clinical monitoring
Use in Specific Populations
- Pregnancy: May cause fetal harm. When pregnancy is recognized, advise the pregnant patient of the risk to a fetus. Discontinue Wegovy® in pregnant patients who are using Wegovy® for weight reduction or at least 2 months before a planned pregnancy
- Lactation: A clinical lactation study reported semaglutide concentrations below the lower limit of quantification in human breast milk. However, salcaprozate sodium (SNAC) and/or its metabolites are present in human milk. Because of the unknown potential for serious adverse reactions in the breastfed infant due to the possible accumulation of SNAC, an absorption enhancer for Wegovy® tablets, and because there are alternative formulations of semaglutide that do not contain SNAC that can be used during lactation, advise patients that breastfeeding is not recommended during treatment with Wegovy® tablets
- Pediatric: Adverse reactions with Wegovy® injection-treated pediatric patients ≥12 years with obesity were similar to those reported in adults. Pediatric patients ≥12 years treated with Wegovy® injection had greater incidences of cholelithiasis, cholecystitis, hypotension, rash, and urticaria compared to adults treated with Wegovy®. There are insufficient data in pediatric patients with T2D treated with Wegovy® injection for obesity to determine if there is an increased risk of hypoglycemia with Wegovy® injection treatment similar to that reported in adults.
The safety and effectiveness of Wegovy® injection have not been established in pediatric patients to reduce the risk of major adverse CV events or to reduce excess body weight and maintain weight reduction long term with the 7.2 mg once weekly dosage or in those <12 years.
The safety and effectiveness of Wegovy® tablets have not been established in pediatric patients - Geriatric: In the CV outcomes trial, patients ≥75 years reported more hip and pelvis fractures on Wegovy® injection than placebo. Patients ≥75 years (Wegovy® injection and placebo) reported more serious adverse reactions overall compared to younger adult patients
- Type 2 Diabetes: Wegovy® tablets have not been studied for weight reduction in adults with T2D and obesity or overweight. Administration of Wegovy® injection resulted in less weight reduction in patients with T2D and obesity or overweight compared to those without T2D and obesity or overweight
Please click here for Wegovy® Prescribing Information, including Boxed Warning.
Indications and Usage
Wegovy® (semaglutide) injection is indicated in combination with a reduced calorie diet and increased physical activity:
- To reduce the risk of major adverse cardiovascular (CV) events (CV death, non-fatal myocardial infarction, or non-fatal stroke) in adults with established CV disease and either obesity or overweight
- To reduce excess body weight and maintain weight reduction long term in:
- Adults and pediatric patients 12 years and older with obesity
- Adults with overweight in the presence of at least one weight-related comorbidity
Wegovy® (semaglutide) tablets are indicated in combination with a reduced calorie diet and increased physical activity to:
- Reduce the risk of major adverse cardiovascular (CV) events (CV death, non-fatal myocardial infarction, or non-fatal stroke) in adults with established CV disease and either obesity or overweight
- Reduce excess body weight and maintain weight reduction long term in adults with obesity or with overweight in the presence of at least one weight-related comorbidity
Limitations of Use:
Concomitant use of Wegovy® tablets or Wegovy® injection with other semaglutide-containing products or with any GLP-1 receptor agonist is not recommended
References
- Wegovy® [package insert]. Plainsboro, NJ: Novo Nordisk Inc.
- Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and cardiovascular outcomes in obesity without diabetes. N Engl J Med. 2023;389(24):2221-2232.
- Data on file. Novo Nordisk Inc.; Plainsboro, NJ.
- FDA approves first treatment to reduce risk of serious heart problems specifically in adults with obesity or overweight. FDA. Published March 8, 2024. Accessed November 5, 2025. https://www.fda.gov/news-events/press-announcements/fda-approved-first-treatment-reduce-risk-serious-heart-problems-specifically-adults-obesity-or
- Khafagy R, Dash S. Obesity and cardiovascular disease: the emerging role of inflammation. Front Cardiovasc Med. 2021;8:768119.
- Ryan DH, Yockey SR. Weight loss and improvement in comorbidity: differences at 5%, 10%, 15%, and over. Curr Obes Rep. 2017;6(2):187-194.
- Zabor EC, Kaizer AM, Hobbs BP. Randomized controlled trials. Chest. 2020;158(1S):S79-S87.
- Sheldrick RC. Randomized trials vs real-world evidence: how can both inform decision-making? JAMA. 2023;329(16):1352-1353.
- Dang A. Real-world evidence: a primer. Pharmeceut Med. 2023;37(1):25-36.
- Smolderen KG, Mena-Hurtado C, Zhao Z, et al. Lower risk of cardiovascular events in patients initiated on semaglutide 2.4 mg in the real-world; results from the SCORE study (Semaglutide Effects on Cardiovascular Outcomes in People with Overweight or Obesity in the Real World). Diabetes Obes Metab. 2025;1-14.