Could once-weekly Sogroya® make a difference for your pediatric patients (2.5 and older) with ISS, NS, or born SGA?

Idiopathic Short Stature (ISS)

Small for Gestational Age (SGA)

Noonan Syndrome (NS)
Pediatric patients (2.5 and older) with
Idiopathic Short Stature (ISS)
Sogroya® demonstrated similar efficacy to daily GH treatment, with fewer injections1
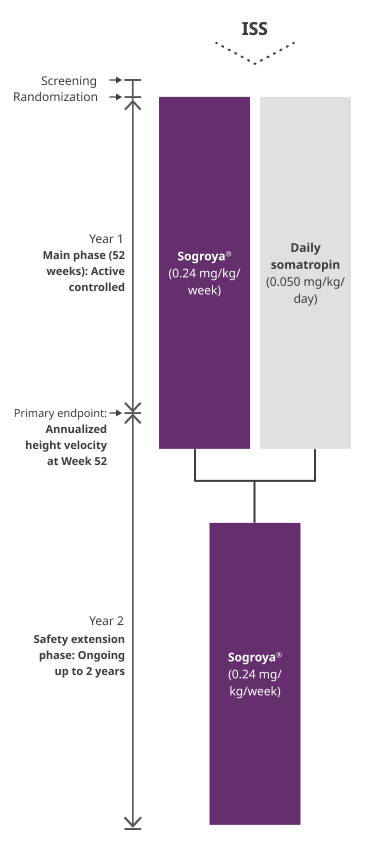
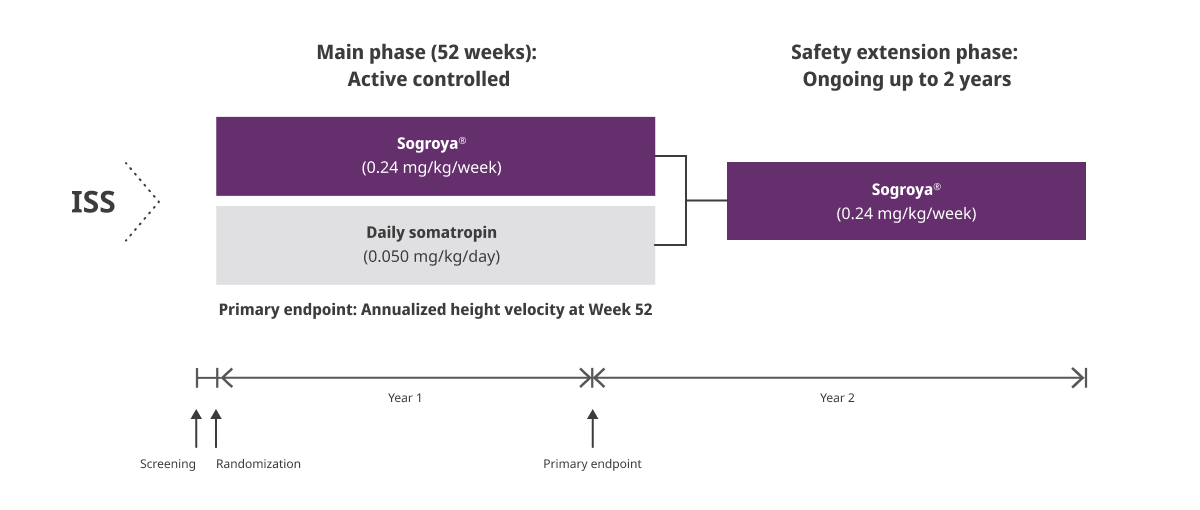
REAL8 main phase: Primary endpoint AHV at Week 521,2
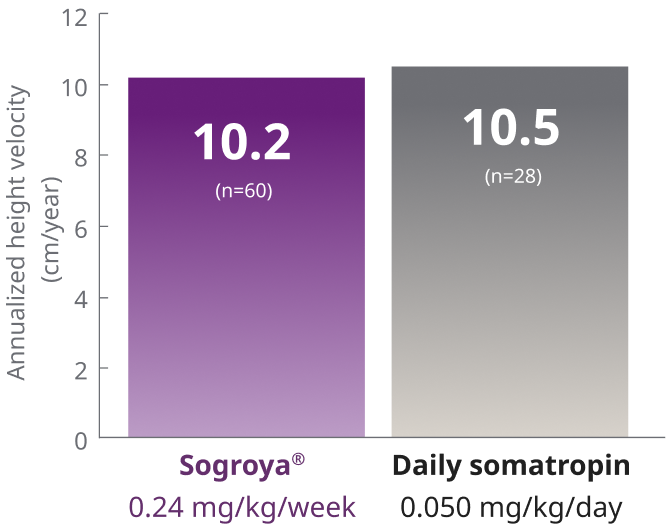
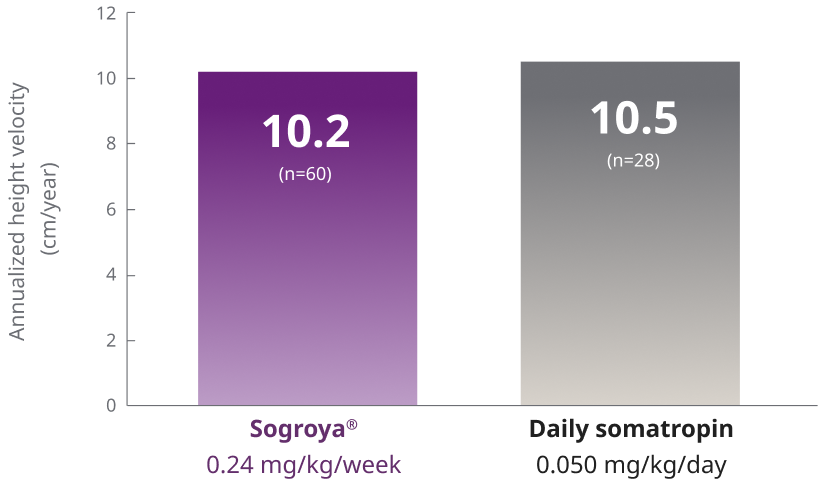
ETD (95% CI) = –0.3 (–1.0; 0.42)
Recommended dosage of Sogroya® for ISS2

REAL8 was a global, multicenter, randomized, open-label, active-comparator, phase 3 basket study. A total of 88 GH-treatment-naïve children 2.8-10.8 years with ISS were randomized to Sogroya® 0.24 mg/kg/week (n=60) or daily somatropin 0.05 mg/kg/day (n=28). Dose 0.05 mg/kg/day of daily somatropin is less than the maximum dose (0.067 mg/kg/day) approved for use in pediatric patients with ISS in the US. The primary endpoint was AHV at Week 52.1
AHV=annualized height velocity; CI=confidence interval; ETD=estimated treatment difference; GH=growth hormone; ISS=Idiopathic Short Stature.
Proven safety profile1
REAL8 main phase: Adverse reactions occurring ≥10% in Sogroya® or somatropin-treated pediatric patients (52 weeks)1


aRespiratory tract infection in the Sogroya® treatment group included influenza (16.9%), upper respiratory tract infection (6.8%), respiratory tract infection (3.4%), pneumonia (1.7%), pneumonia bacterial (1.7%), respiratory tract infection viral (1.7%), and viral upper respiratory tract infection (1.7%).
bNasopharyngitis in the Sogroya® treatment group included nasopharyngitis (15.3%), pharyngitis streptococcal (5.1%), pharyngitis (1.7%), rhinitis (1.7%), sinusitis (1.7%), and tracheitis (1.7%).
cEar infection in the Sogroya® treatment group included otitis media (6.8%), ear infection (3.4%), and otitis media acute (1.7%).
dDiarrhea in the Sogroya® treatment group included gastroenteritis (3.4%), gastroenteritis viral (3.4%), diarrhea (1.7%), enterobiasis (1.7%), and parasitic gastroenteritis (1.7%).
eInjection-site reaction in the Sogroya® treatment group included application-site reaction (1.7%), injection-site bruising (1.7%), injection-site hematoma (1.7%), injection-site hemorrhage (1.7%), injection-site pruritis (1.7%), a n d injection-site urticaria (1.7%).
fCough in the Sogroya® treatment group included cough (5.1%).
gVomiting in the Sogroya® treatment group included vomiting (5.1%).
ISI=Idiopathic Short Stature.


REAL8: A global, multicenter, randomized, open-labeled, active-comparator, phase 3 basket study1
ISS= Idiopathic Short Stature.
Pediatric patients (2.5 and older) born
Small for Gestational Age (SGA)
with no catch-up growth by 2 years of age
Sogroya®: Non-inferior efficacy with fewer injections compared with daily GH1
REAL8 main phase: Primary endpoint AHV at Week 521,2


Recommended dosage of Sogroya® for SGA2

REAL8 was a global, multicenter, randomized, open-label, active-comparator, phase3 basket study. A total of 142 GH-treatment-naïve children 2.6-10.7 years born SGA were randomized to Sogroya® 0.24 mg/kg/week (n=70) daily somatropin 0.035 mg/kg/day (n=37), or daily somatropin 0.067 mg/kg/day (n=35). Dose 0.035 mg/kg/day of daily somatropin is less than the maximum dose (0.067 mg/kg/day) approved for use in pediatric patients with SGA in the US. The primary endpoint was AHV at Week 52.1
AHV=annualized height velocity; CI=confidence interval; ETD=estimated treatment difference; GH=growth hormone; IGF-1=insulin-like growth factor; SGA=Small for Gestational Age.
Proven safety profile1
REAL8 main phase: Adverse reactions occurring ≥10% in Sogroya® or somatropin-treated pediatric patients (52 weeks)1


hNasopharyngitis in the Sogroya® treatment group included nasopharyngitis (15.9%), pharyngitis (2.9%), rhinitis (2.9%), pharyngitis streptococcal (1.4%), sinusitis (1.4%), and viral rhinitis (1.4%).
iRespiratory tract infections in the Sogroya® treatment group included upper respiratory tract infection (20.3%), influenza (10.1 %), metapneuomovirus infection (1.4%), mycoplasma infection (1.4%), pneumonia (1.4%), pneumonia bacterial (1.4%), pneumonia mycoplasmal (1.4%), respiratory syncytial virus infection (1.4%), and respiratory tract infection (1.4%).
jCough in the Sogroya® treatment group included cough (15.9%).
kEar infection in the Sogroya® treatment group included otitis media (7.2%), ear infection (2.9%), otitis externa (1.4%), and otitis media acute (1.4%).
lDiarrhea in the Sogroya® treatment group included diarrhea (4.3%), gastroenteritis (4.3%), and gastrointestinal viral infection (1.4%).
mVomiting in the Sogroya® treatment group included vomiting (10.1%).
SGA=Small for Gestational Age.

REAL8: A global, multicenter, randomized, open-labeled, active-comparator, phase 3 basket study1


SGA=small for gestational age.
Pediatric patients (2.5 and older) with
Noonan Syndrome (NS)
Sogroya® demonstrated similar growth with fewer injections when compared with daily GH1
REAL8 main phase: Primary endpoint AHV at Week 521,2


ETD (95% CI) = 1.2 (0.32; 2.03)
Recommended dosage of Sogroya® for NS2

REAL8 was a global, multicenter, randomized, open-label, active-comparator, phase 3 basket study. A total of 77 GH-treatment-naïve children 2-11.1 years with NS were randomized to Sogroya® 0.24 mg/kg/week (n=49) or daily somatropin 0.05 mg/kg/day (n=28). Dose 0.05 mg/kg/day of daily somatropin is less than the maximum dose (0.066 mg/kg/day) approved for use in pediatric patients with NS in the United States. The primary endpoint was AHV at Week 52.1
AHV=annualized height velocity; CI=confidence interval; ETD=estimated treatment difference; GH=growth hormone; NS=Noonan Syndrome.
Proven safety profile1
REAL8 main phase: Adverse reactions occurring ≥10% in Sogroya® or somatropin-treated pediatric patients (52 weeks)1


nRespiratory tract infection in the Sogroya® treatment group included upper respiratory tract infection (20.4%), influenza (10.2%), pneumonia (6.1 %), influenza like illness (2%), respiratory syncytial virus infection (2%), respiratory tract infection (2%), respiratory tract infection viral (2%), upper respiratory tract infection bacterial (2%), and viral upper respiratory tract infection (2%).
oNasopharyngitis in the Sogroya® treatment group included nasopharyngitis (24.5%), pharyngitis (4.1 %), bacterial infection (2%), herpes pharyngitis (2%), pharyngitis streptococcal (2%), pharyngotonsillitis (2%), and rhinitis (2%).
pDiarrhea in the Sogroya® treatment group included gastroenteritis (14.3%), diarrhea (6.1%), gastroenteritis viral (2%), and parasitic gastroenteritis (2%).
qEar infection in the Sogroya® treatment group included otitis media (8.2%), otitis externa (4.1 %), ear infection (2%), otitis media acute (2%), and otitis media chronic (2%).
rCough in the Sogroya® treatment group included cough (12.2%) and bacterial infection (2%).
sVomiting in the Sogroya® treatment group included vomiting (8.2%) and gastritis (4.1%).
tInjection site reaction in the Sogroya® treatment group included injection site bruising (6.1%) and injection site hemorrhage (2%).
uAbdominal pain in the SOGROYA treatment group included abdominal distension (2%).
NS=Noonan Syndrome.

REAL8: A global, multicenter, randomized, open-labeled, active-comparator, phase 3 basket study1


NS=Noonan Syndrome.
Other specific growth-related conditions: IGF-1 Response
Explore IGF-1 response for pediatric patients with other specific growth-related conditions.

Dosing for pediatric patients
See dosing information for switch and treatment-naïve patients.