
Most patients and caregivers preferred the Sogroya® pen over Skytrofa® auto-injector and Ngenla® pen1,3,c
Results from a randomized, crossover study assessing device preference and ease of use following simulated injections with the Sogroya® pen and Skytrofa® auto-injector or Ngenla® pen.

preferred the Sogroya® pen over Skytrofa® auto-injector3,c
(14% preferred Skytrofa® auto-injector; 7% had no preference between devices)

Sogroya® pen was easy or very easy to use3,c
(57% considered Skytrofa® auto-injector easy or very easy to use)

preferred Sogroya® pen over Ngenla® pen1,c
(13% preferred Ngenla® pen; 3% had no preference between devices)

Sogroya® pen was easy or very easy to use1,c
(74% considered Ngenla® pen easy or very easy to use)

preferred the Sogroya® pen over Skytrofa® auto-injector3,c
(14% preferred Skytrofa® auto-injector; 7% had no preference between devices)

Sogroya® pen was easy or very easy to use3,c
(57% considered Skytrofa® auto-injector easy or very easy to use)

preferred Sogroya® pen over Ngenla® pen1,c
(13% preferred Ngenla® pen; 3% had no preference between devices)

Sogroya® pen was easy or very easy to use1,c
(74% considered Ngenla® pen easy or very easy to use)

Results based on two open-label, multicenter, randomized, crossover studies of the same design. One study compared the handling of Sogroya® pen vs Ngenla® pen in 70 participants, naïve to both or similar devices: 33 adolescents with growth-related disorders aged 10 to 17 years, and 37 caregivers ≥18 years of age. The other study compared the handling of Sogroya® pen vs Skytrofa® auto-injector in 70 participants, naïve to both or similar devices: 35 adolescents with growth-related disorders aged 10 to 17 years, and 35 caregivers ≥18 years of age. The primary objective of both studies was to evaluate patient device preference as measured by the Device Handling and Preference Assessment Questionnaire (DHPAQ). Another objective was to compare the ease of use of the 2 devices included in the study. Other endpoints included device training time, preparation and injection time, and overall number of complete injections. After receiving training for both devices included in the study, participants performed a simulated injection into a pad or mannequin and completed the DHPAQ. Confirmatory validation of the DHPAQ was done via postinjection cognitive interviews, confirming that the DHPAQ was comprehensive, relevant to their experiences, and fully comprehended by the participants.1,3
Limitations: A US-only, small sample size participant pool of 2 distinct groups, potentially reducing statistical power. Adolescents were not required to be injection naïve and children under 10 years were excluded. Assessment of treatment adherence or adverse events was not done. The studies took place in a controlled setting with assessment at a single time point, not reflecting long-term use.
cThese data do not establish clinical comparability of the products for any indications and should not be seen as making any claim regarding efficacy and safety. These data make no representation or conclusion as to the factors contributing to patient preference. All percentages have been rounded to the nearest whole number.
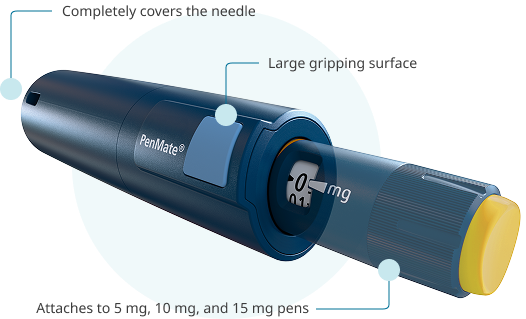
PenMate® keeps needles out of sight
Now approved for Sogroya®, PenMate® is a reusable cover for the 5 mg, 10 mg, and 15 mg pens. Once attached to the end of a pen, it completely covers the needle, keeping it unseen as it enters the skin. PenMate® also has a large gripping surface for holding firmly.
Patients can order their PenMate® by contacting their NovoCare® Case Manager or by calling 1‑888‑668‑6444.
Pediatric dosing
See dosing information for switch and treatment-naïve patients alike.
See dosing information for switch and treatment-naïve patients alike.
Device attribute chart
Learn about select features of the Sogroya® pen and other growth hormone therapy devices.
Learn about select features of the Sogroya® pen and other growth hormone therapy devices.