WHY A ONCE-WEEKLY THERAPY?
WHY A ONCE-WEEKLY THERAPY?
Understand what obstacles may present for patients and caregivers
Understand how growth hormone deficiency (GHD) can affect pediatric and adult patients.

Missing multiple daily injections per week may substantially impact growth outcomes1
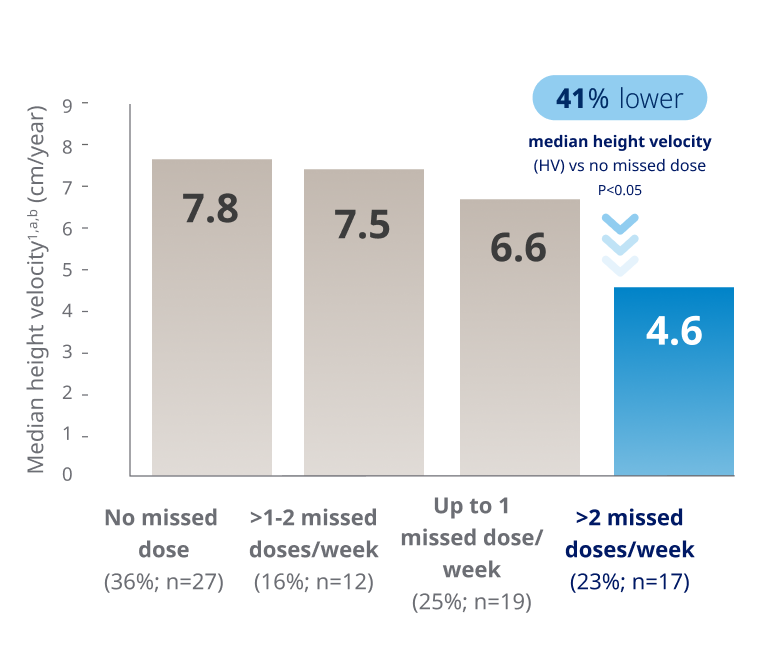
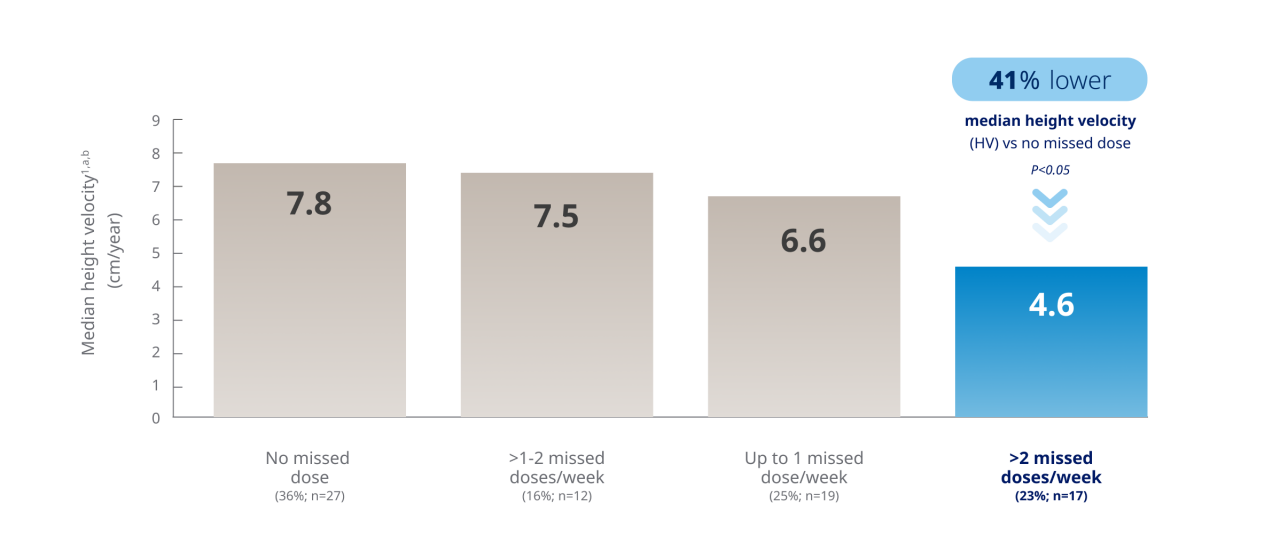
Chart based on Kapoor RR, et al. Monitoring of concordance in growth hormone therapy. Arch Dis Child. 2008;93(2):147-148.
Patients who missed >2 injections per week had a 41% lower median HV than those who missed none1,a,b
- Factors associated with lower adherence to therapy were a longer duration on GH therapy, lack of choice over GH device, and short duration (<4 weeks) of GH prescriptions
aUK study of 75 children with GHD who received GH therapy and attended a regional pediatric endocrine clinic from 1999 to 2003. 58 general practitioners (GPs) who issued GH prescriptions responded to a mailed questionnaire (66 GPs were contacted; 88% response rate) with the number of issued prescriptions and the total GH dose (or number of vials/cartridges) issued with each prescription during 3 specific 12-month periods (1999-2000, 2000-2001, and 2002-2003). Data on 11 patients were obtained from an outreach clinic where GH prescriptions were provided directly by a designated local consultant pediatrician. Adherence was assessed in each child by comparing total expected GH usage as documented in clinic records and letters to the total amount of GH prescribed by GPs during a 12-month period.1
bAdjusted for age and duration of GH therapy.1
GHD=growth hormone deficiency; HV=height velocity; GH=growth hormone.
In a systematic literature review and meta-analysis of medication adherence with once-weekly vs once-daily therapy,
Once-weekly treatment adherence was ~2X better than once-daily treatment2,c
cMeta-analysis of observational studies which were conducted in patients with osteoporosis.2
According to an LAGH Consensus Statement for pediatric GHD patients, developed independently by a panel of renowned pediatric endocrinology experts3:
- LAGH formulations offer a potential advantage over daily GH injections for children with GH deficiency in terms of reduced injection frequency and treatment burden; this may also be associated with improved adherence and treatment outcomes over time. However, long-term data is needed
- Parents/caregivers have shown a strong preference for the reduced frequency of LAGH preparations over daily GH formulations
- It is likely that most if not all children could be considered for a weekly administration regimen, particularly children or their caregivers who experience challenges with injections, as well as those at increased risk of non-adherence, frequent travel schedules, and split households


Consider if the flexibility of a once-weekly GH treatment option may impact your patient’s persistence and treatment experience
GH=growth hormone; GHD=growth hormone deficiency; LAGH=long-acting growth hormone.
Daily injections may present obstacles for patients and their caregivers
Patients with GHD continue to face challenges with daily injections4
Non-adherence to daily GH treatment is common and has been addressed in many studies5,6
Repeated injections are one of the main causes of non-adherence in pediatric-aged patients7

Children, adolescents, and their caregivers may struggle with continual daily injections over the long term4
Missed daily injections may impact growth outcomes8
GHD=growth hormone deficiency; GH=growth hormone
Missing
1 DAY
per week of daily
GH treatment
results in missing up to
52 DAYS
of treatment
in a year
which equates to missing
~1 YEAR
of doses over a 7-year
treatment period
GHD occurs in adults and has associated symptoms and conditions
Adult GHD (AGHD) is most often acquired from9,10:

A pituitary tumor9,10
Including treatment with surgery and/or radiation10

Trauma to the brain9
Other patient subpopulations include subarachnoid hemorrhage, ischemic stroke, and infections in the central nervous system9
AGHD may also be idiopathic or due to other organic causes.9,10
Symptoms and associated conditions of adult GHD include9:
Reduced energy levels
Reduced muscle strength
Osteoporosis
Lipid abnormalities
Increased total body fat

Insulin resistance
Impaired cardiac function
Symptoms and associated conditions of adult GHD include9:
Reduced energy levels
Reduced muscle strength
Osteoporosis
Lipid abnormalities
Increased total body fat

Insulin resistance
Impaired cardiac function
Management of adult GHD
Per the American Association of Clinical Endocrinologists (AACE), identifying adult patients with GHD includes assessing10:
PATIENTS WITH CLINICAL FEATURES SUGGESTIVE OF AGHD
eg, patients with organic hypothalamic-pituitary disease and low-serum IGF-1 levels
BIOCHEMICALLY PROVEN
EVIDENCE OF AGHD
eg, GH stimulation testing
Treatment options4,10
- With diagnosis confirmed, AACE recommends treating AGHD with growth hormone therapy10
- While once-daily GH treatment is considered the standard of care, according to GRS consensus, a once-weekly GH option may also help4
AGHD=adult growth hormone deficiency; GH=growth hormone; GHD=growth hormone deficiency; GRS=Growth Hormone Research Society; IGF-1=insulin-like growth factor-1.
How might treatment adherence affect pediatric patients with other specific growth-related conditions?
Early initiation and adherence to GH therapy may lead to improved growth outcomes in pediatric patients with ISS4,11-14
Treatment burden in ISS:
Diagnosis and treatment can be delayed, potentially reducing the treatment window15,16
- Average treatment duration is 4 to 7 years14
Treatment drop-out due to poor
adherence is common15
GH=growth hormone; ISS=Idiopathic Short Stature.
For children born SGA who are on GH therapy, treatment fatigue and poor adherence may lead to reduced growth outcomes17,18
Treatment burden in SGA:
In a cohort from an observational French registry study:
≈20% of patients (n=58/291) with SGA prematurely stopped GH treatment before reaching a normalized height17,d
Reasons for premature discontinuation included safety concerns, poor adherence, satisfaction with attained height, and patient, parent, or physician decision17
SGA can be associated with multiple comorbidities, which may increase treatment burden19,20

Parents of newborns born SGA may experience higher levels of psychological burden compared to those born normal for gestational age.21
dBased on an observational, multicenter, non-interventional French registry study that assessed the effectiveness and safety of daily GH in 1408 French children born SGA from 2005 to 2010. A cohort of 291 children were randomly selected for every fifth patient in the main study population to be followed for up to 6 months after the first visit and then annually until achieving final adult height or study termination. Final adult height was defined as height velocity <2 cm/year or bone age >14 years for girls and >16 years for boys. Normalized height was defined as height SDS >-2 from the reference population.
GH=growth hormone; SDS=standard deviation score; SGA=Small for Gestational Age.
Children with NS face a complex treatment burden, which may impact medication adherence22,23
Treatment burden in NS:
NS is a lifelong, multisystem condition with diverse complications and comorbidities that requires multidisciplinary care24,25
Late diagnosis may limit their GH treatment window22

Data suggest poor adherence to daily GH therapy may lead to a reduced height velocity for patients with NS23
GH=growth hormone; NS=Noonan Syndrome.
Missing 1 day per week of daily GH treatment is equivalent to missing 52 days of treatment in a year. If the treatment period is 7 years, this equates to skipping a full year of treatment.
Discover the pen
Discover the pen
Take a look at the features of the Sogroya® pen.

Take a look at the features of the Sogroya® pen.
How does it work?
How does it work?
Discover the science behind Sogroya®.
Discover the science behind Sogroya®.