Pediatric IGF-1 data
Pharmacodynamic endpoint: IGF-1 response over 52 weeks
Supportive secondary endpoint: Mean IGF-1 SDS levels at Weeks 0 to 522,3,a
Main Phase: IGF-1 SDS levels were –2.03 at baseline and the IGF-1 SDS level change from baseline was +2.362,3



of pediatric patients achieved an average IGF-1 SDS level within normal range after 52 weeks of treatment with Sogroya®, similar to daily somatropin2,3
- Average change of 0.02 mg/kg resulting in a change in IGF-1 standard deviation score (SDS) of 0.32
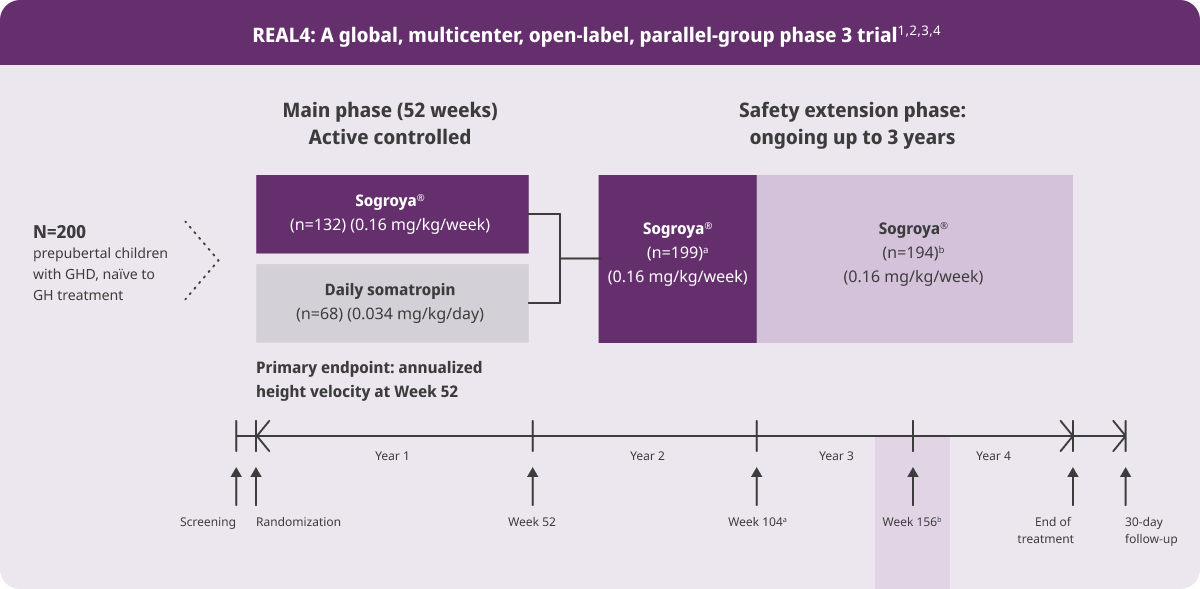
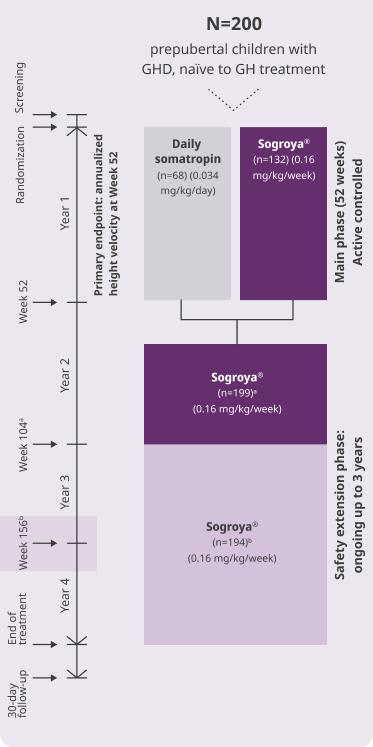
REAL4 is a multicenter, open-label, active-controlled, parallel-group phase 3 trial. A total of 200 treatment-naïve children aged 2.5 to 11 years with a confirmed diagnosis of GHD were randomized 2:1 to receive Sogroya® 0.16 mg/kg/week (n=132) or daily somatropin 0.034 mg/kg/day (n=68). The primary endpoint was annualized height velocity at Week 52.2 See study design.
aWeek 4 and 26 samples were collected in a window designed to characterize the peak between 1 and 4 days after dosing: mean sampling times after dosing were 45 and 44 hours (1.9 and 1.8 days), respectively. Trough samples at Weeks 13 and 39 were taken on Day 7. Week 52 samples taken 4 to 6 days after dosing captured expected weekly averages: mean sampling time after dosing was 113 hours (4.7 days). During the 52-week treatment period, 5 (3.8%) patients on Sogroya® and 2 (2.9%) patients on daily GH had an IGF-1 SDS above +2.0 at two or more consecutive visits. No safety issues were associated with IGF-1 SDS levels >+2.5 in 2 patients.3
GH=growth hormone; GHD=growth hormone deficiency; IGF-1=insulin-like growth factor-1; SDS=standard deviation score.
Pharmacodynamic endpoint: Weekly IGF-1 SDS profile1,3
Main Phase: Supportive secondary endpoint


Graph shows the weekly IGF-1 SDS profile (mean and 5th to 95th percentile) estimated from IGF-1 samples obtained in REAL4, derived by population PK/PD modeling, with a weekly average IGF-1 SDS in the normal range (SDS of –2 to +2) for 97% of patients.1,3
Limitations: It was assumed that missing data (dosing history, PK, and IGF-1) were missing at random. The structural model, interindividual variability model, and covariate model were assumed adequate for the analysis, and this was verified during model qualification. None of these assumptions and limitations were evaluated to affect the model validity.1
Model-based analysis of IGF-1 in children with GHD4,b
This table allows for calculation of estimated average weekly IGF-1 exposure from a single IGF-1 sample obtained at any time within the Sogroya® (0.16 mg/kg/week) dosing interval at steady state. In practice, this tool requires knowledge of Sogroya® injection timing relative to IGF-1 sample collection.4
Calculating
IGF-1avg SDS
Adjustment to measured IGF-1 SDS to approx IGF‑1avg SDS
90% PI of IGF-1 SDS adjustment value
25-48
hours after dose
IGF-1 SDS - 0.8
+/- 0.5
49-72
hours after dose
IGF-1 SDS - 1.0
+/- 0.6
73-96
hours after dose
IGF-1 SDS - 0.5
+/- 0.4
97-120
hours after dose
No adjustmentc
N/A
121-144
hours after dose
IGF-1 SDS + 0.7
+/- 0.4
145-168
hours after dose
IGF-1 SDS + 1.1
+/- 0.6
IGF-1avg conc (ng/mL)
Adjustment to measured IGF-1 (ng/mL) to approx IGF-1avg (ng/mL)
CV (%) of IGF-1 (ng/mL) adjustment value
25-48
hours after dose
IGF-1 (ng/mL) x 0.8
9.0
49-72
hours after dose
IGF-1 (ng/mL) x 0.7
8.3
73-96
hours after dose
IGF-1 (ng/mL) x 0.9
7.4
97-120
hours after dose
No adjustmentc
N/A
121-144
hours after dose
IGF-1 (ng/mL) x 1.3
10.0
145-168
hours after dose
IGF-1 (ng/mL) x 1.6
15.0
Calculating:
IGF-1avg SDS
IGF-1avg conc (ng/mL)
Interval
(hours after dose)
Adjustment to measured IGF-1 SDS to approx IGF‑1avg SDS
90% PI of IGF-1 SDS adjustment value
Adjustment to measured IGF-1 (ng/mL) to approx IGF-1avg (ng/mL)
CV (%) of IGF-1 (ng/mL) adjustment value
25-48
IGF-1 SDS - 0.8
+/- 0.5
IGF-1 (ng/mL) x 0.8
9.0
49-72
IGF-1 SDS - 1.0
+/- 0.6
IGF-1 (ng/mL) x 0.7
8.3
73-96
IGF-1 SDS - 0.5
+/- 0.4
IGF-1 (ng/mL) x 0.9
7.4
97-120
No adjustmentc
N/A
No adjustmentc
N/A
121-144
IGF-1 SDS + 0.7
+/- 0.4
IGF-1 (ng/mL) x 1.3
10.0
145-168
IGF-1 SDS + 1.1
+/- 0.6
IGF-1 (ng/mL) x 1.6
15.0

IGF-1 steady state reached within 1 to 2 doses after initiating Sogroya®4
bPK/PD modeling analyses included dosing information and 1473 PK samples from 210 Sogroya®-treated pediatric patients with GHD across 3 trials (phase1, phase 2 [REAL3], and phase 3 [REAL4]), as well as 1381 IGF-1 samples from 186 Sogroya®-treated pediatric patients with GHD in REAL3 and REAL4. Throughout REAL3 and REAL4, serial blood sampling was performed before first dose, 1 to 4 days and 4 to 6 days after dosing and before next dose to cover baseline, maximum (peak), estimated weekly average, and minimum (trough) PK as well as IGF-1 concentrations.
cAdjustment for values obtained 97 to 120 hrs after dose is considered not to be required as the predicted adjustments of IGF-1 SDS + 0.1 (PI 90% ± 0.3 SDS) and IGF-1 (ng/mL) x 1.1 (6.9 CV%) are not clinically relevant.
avg=average; approx=approximate; conc=concentration; CV=coefficient of variation; GHD=growth hormone deficiency; IGF-1=insulin-like growth factor-1; PD=pharmacodynamic; PK=pharmacokinetic; PI=prediction interval; SDS=standard deviation score.
Limitations: Results should always be interpreted in the context of individual clinical management.
If steady state has not been achieved at the time of sampling and/or if the Sogroya® dose is changed, this is not accounted for within the linear model, and subsequent predictions of IGF-1 values may be biased.
Analysis results may vary from 1 sample to another due to technical reasons, such as assay variability, pharmacological reasons, such as dose-to-dose variation in bioavailability, and temporal variations in physiology, which may affect the accuracy of IGF-1 sampling and limit the predictive power of the model.
For START and SWITCH groups, IGF-1 exposure was within normal range (–2 to +2) at 2 years1
Extension Phase: Mean IGF-1 SDS levels at Week 104 (supportive secondary endpoint)1,5,d

- Model-derived IGF-1 SDS suggests similar mean average IGF-1 SDS levels over the weekly dosing interval within normal range (–2 to +2 SDS) in Year 1 and for both groups (+0.72 and +0.75 for the START [Sogroya®/Sogroya®] and SWITCH [daily GH/Sogroya®] groups, respectively) in Year 25
- Overall, IGF-1 levels greater than +2 SDS were measured in 28 (21.7%) and 10 (14.7%) patients in the START (Sogroya®/ Sogroya®) and SWITCH (daily GH/Sogroya®) groups, respectively, during the Week 52 to Week 104 period5
- This surpassing of +2 SDS occurred on 2 consecutive visits in 1 (0.8%) and 2 (3.1%) of the patients in the START and SWITCH groups, respectively. This may be due to a discrepancy in the actual timing of IGF-1 SDS sampling between the groups5
- No trend was seen in the amount or type of AEs reported in patients with IGF-1 levels greater than +2 SDS5
The REAL4 main trial phase (Week 0 to Week 52) was followed by an ongoing 3-year, single-group, safety extension phase (Week 52 to Week 208). The 2-year data presented here represent up to Week 104. A total of 199 patients rolled over into the safety extension where all patients received Sogroya® 0.16 mg/kg/week, either continuing Sogroya® treatment (START patients) or switching from daily GH treatment in main phase to once-weekly Sogroya® (SWITCH patients). 194 of 199 patients completed at 104 weeks of treatment (127 START patients and 67 SWITCH patients). No statistical analyses of data were performed during the extension phase. The observations after Week 52 to Week 104 are presented using descriptive statistics.1,5
dBlood samples for IGF-1 measurements in patients treated with somapacitan up to Week 104 were taken at the following time points after dosing: Week 4, Week 26, and Week 78 (Days 1-4 after dosing; around peak level), Week 13, Week 39, and Week 104 (Day 7 after dosing; trough level) and at Week 52 (Days 4-6 after dosing; expected weekly average IGF-1 SDS). The number of patients that at some time during the second year had an IGF-1 SDS value exceeding +2.5 was 15 (11.6%) and 4 (5.9%) in the start and switch groups, respectively. None of these patients had a IGF-1 value exceeding +2.5 SDS at 2 consecutive visits.5
AE=adverse event; GH=growth hormone; GHD=growth hormone deficiency; IGF-1=insulin-like growth factor-1; SDS=standard deviation score.
IGF-1 exposure was maintained within normal range (–2 to +2) at 3 years1
Extension Phase: Mean IGF-1 SDS levels at Week 156 (supportive secondary endpoint)1,e

- Model-derived IGF-1 SDS suggests similar mean average IGF-1 SDS levels over the weekly dosing interval within normal range (–2 to +2 SDS) throughout 156 weeks for both groups with the mean (SD) IGF-1 SDS levels of –0.24 (1.10) for the START (Sogroya®/Sogroya®) and –0.34 (1.34) for the SWITCH (daily GH/Sogroya®) groups1
- IGF-1 levels were taken at Week 156 on Day 7 (approximate trough level) and data were missing for 2 participants in the START group and 3 participants in the SWITCH groups1
- No trend was seen in the amount or type of AEs reported in patients with IGF-1 levels greater than +2 SDS1
The REAL4 main trial phase (Week 0 to Week 52) was followed by an ongoing 3-year, single-group, safety extension phase (Week 52 to Week 208). The 3-year data presented here represent up to Week 156. A total of 194 patients continued in the safety extension where all patients received Sogroya® 0.16 mg/kg/week, either continuing Sogroya® treatment (START patients) or switching from daily GH treatment in the main phase to once-weekly Sogroya® (SWITCH patients). 188 of 194 patients completed 156 weeks of treatment (125 START patients and 63 SWITCH patients). No statistical analyses of data were performed during the extension phase. The observations from Week 52 to Week 156 are presented using descriptive statistics.1
eBlood samples for IGF-1 measurements in subjects treated with somapacitan up to Week 156 were taken at the following time points: Week 4, Week 26, Week 78, and Week 130 (Days 1-4 after dosing; around peak IGF-1 level), Week 13, Week 39, Week 104, and Week 156 (Day 7 after dosing; around trough IGF-1 level) and at Week 52 (Days 4-6 after dosing; around average IGF-1 level). The number of participants that at some time during Year 3 had an IGF-1 value exceeding +2.5 SDS was 13 (10.4%) and 3 (4.7%) in the START and SWITCH groups, respectively, with participants exceeding +3.0 SDS were 1 (0.8%) and 0 (0%), respectively. One participant (0.8%) in the START group had an IGF-1 value exceeding +2.5 SDS at 2 consecutive visits.1
AE=adverse event; GH=growth hormone; GHD=growth hormone deficiency; IGF-1=insulin-like growth factor-1; SDS=standard deviation score.
Adults reached favorable IGF-1 levels
Sogroya® achieved serum IGF-1 increases that were comparable to daily treatment2
Secondary endpoint: IGF‑1 SDS values2,6
Baseline


Week 34


Draw IGF-1 samples 3 to 4 days after the prior dose.2
In a 35-week, double-blind, placebo-controlled study, 300 treatment-naïve adult patients with GHD (full analysis set) were randomized (2:1:2) to once-weekly Sogroya® 10 mg/1.5 mL (n=120), once-weekly placebo (n=61), or daily somatropin 10 mg/1.5 mL (n=119) for a 34-week treatment period.2 See study design.
GHD=growth hormone deficiency; IGF-1=insulin-like growth factor-1; SDS=standard deviation score.