
Powerful glycemic control with compelling weight loss with Ozempic® (semaglutide) injection1
Ozempic® is not indicated for weight loss


Ozempic® vs Lantus® and Ozempic® 1 mg vs 2 mg1
Primary endpoint:
change in A1C from baseline
SUSTAIN 4:
vs study-titrated Lantus®1,5
In insulin-naïve adult patients with type 2
diabetes on metformin ± sulfonylurea
Mean change in A1C from baseline at Week 30
Mean baseline A1C:
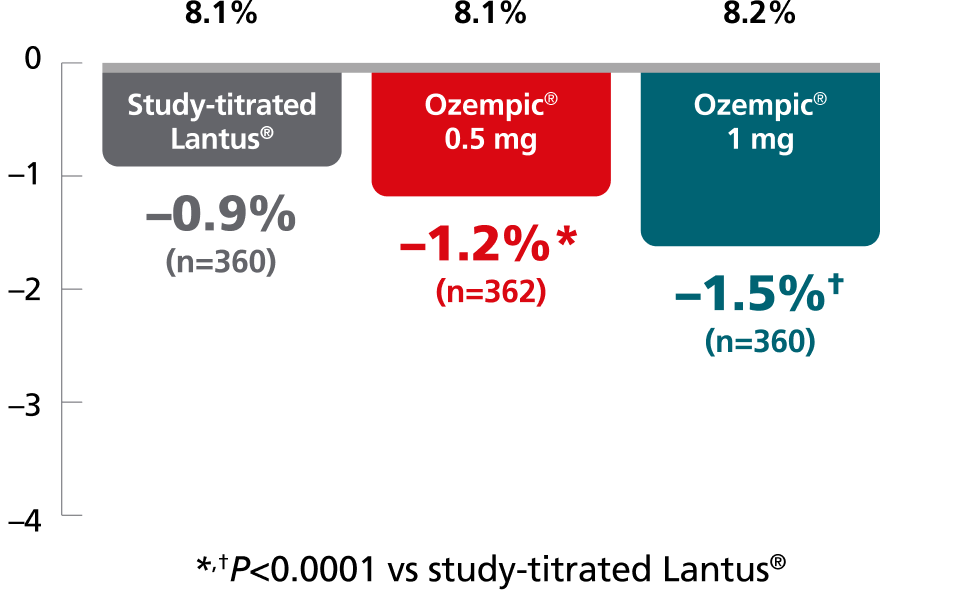
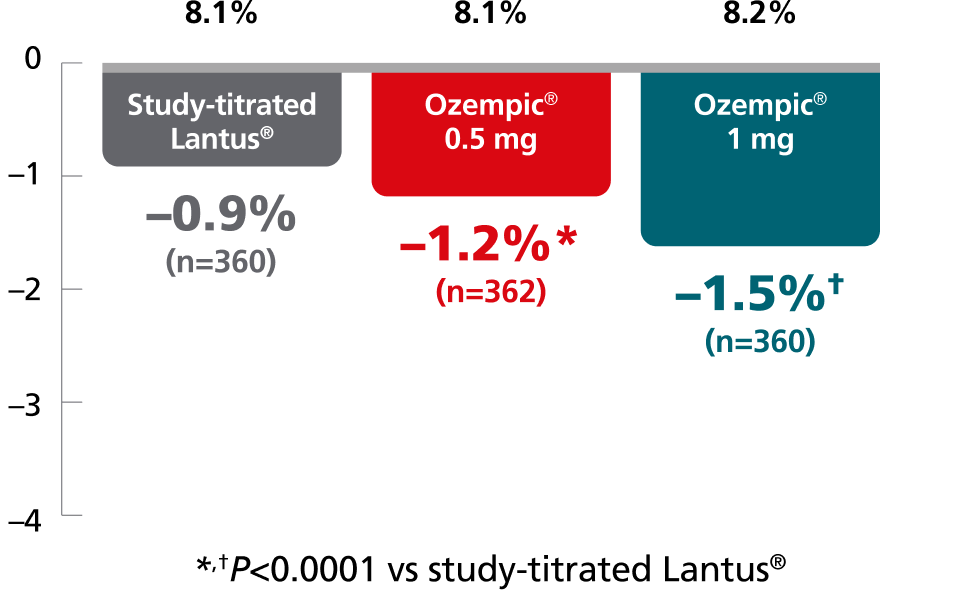
26% of insulin patients titrated to goal by Week 30.
Mean daily insulin dose: 29 U/day
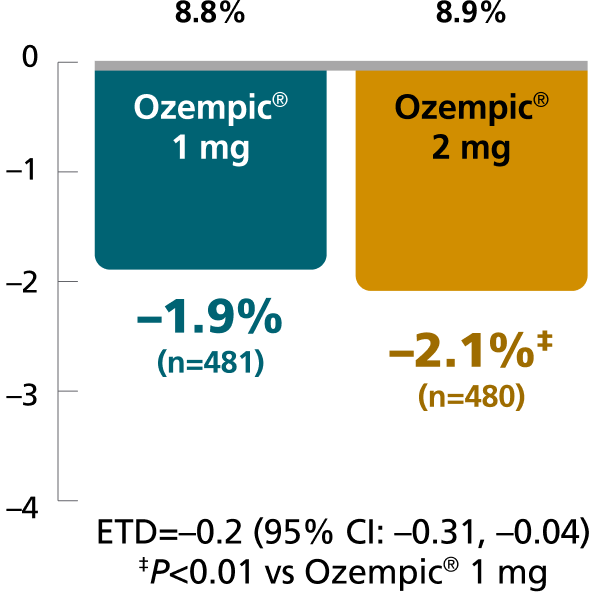
SUSTAIN FORTE:
Ozempic® 1 mg vs 2 mg1,4,8
In patients with type 2 diabetes on
metformin ± sulfonylurea
Mean change in A1C from baseline at Week 40
Mean baseline A1C:
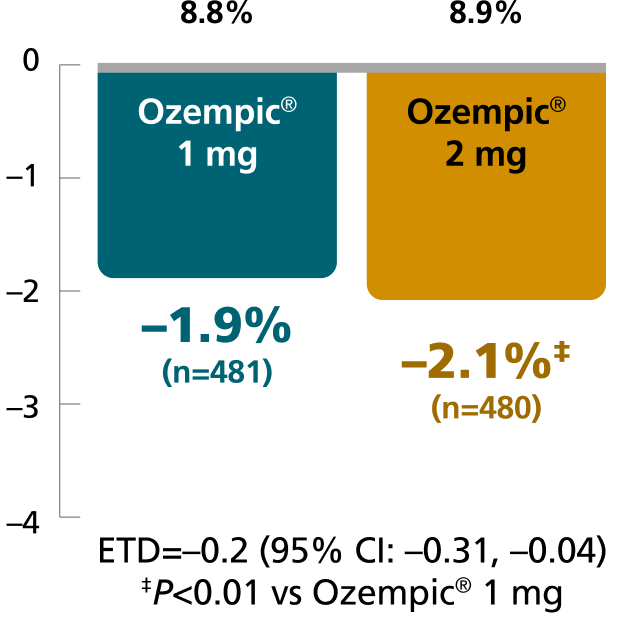
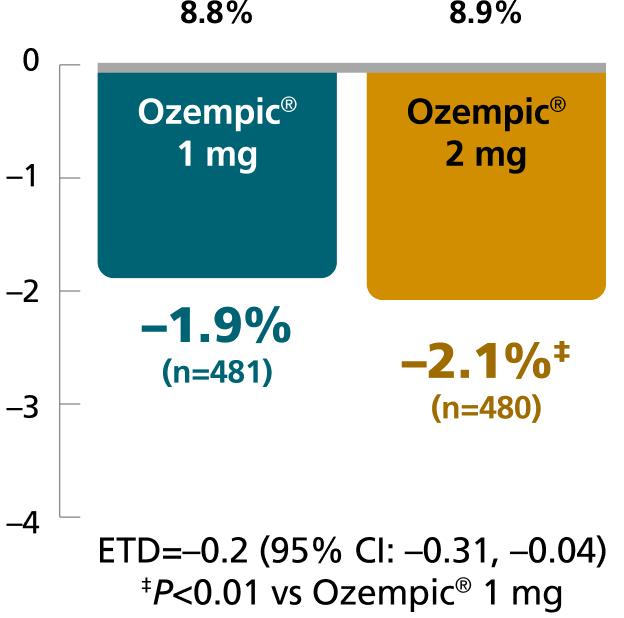
Results for SUSTAIN 4 and SUSTAIN FORTE are based on sensitivity analyses of retrieved dropout population.
SUSTAIN 4: A 30-week, randomized, open-label, active-controlled trial in 1089 insulin-naïve adult patients on metformin ± sulfonylurea with type 2 diabetes comparing Ozempic® injection 0.5 mg and Ozempic® injection 1 mg with Lantus®.9
SUSTAIN FORTE: A 40-week, randomized, active-controlled trial in 961 adult patients with type 2 diabetes on metformin with or without a sulfonylurea, comparing Ozempic® injection 1 mg with Ozempic® injection 2 mg.1,4
SUSTAIN 4:
vs study-titrated Lantus®1,9
In insulin-naïve adult patients with type 2 diabetes
on metformin ± sulfonylurea
Percent of patients who achieved A1C <7% at Week 30
Mean baseline A1C:
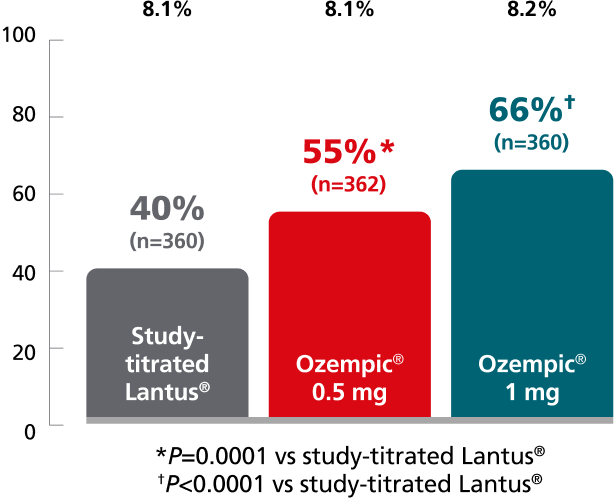
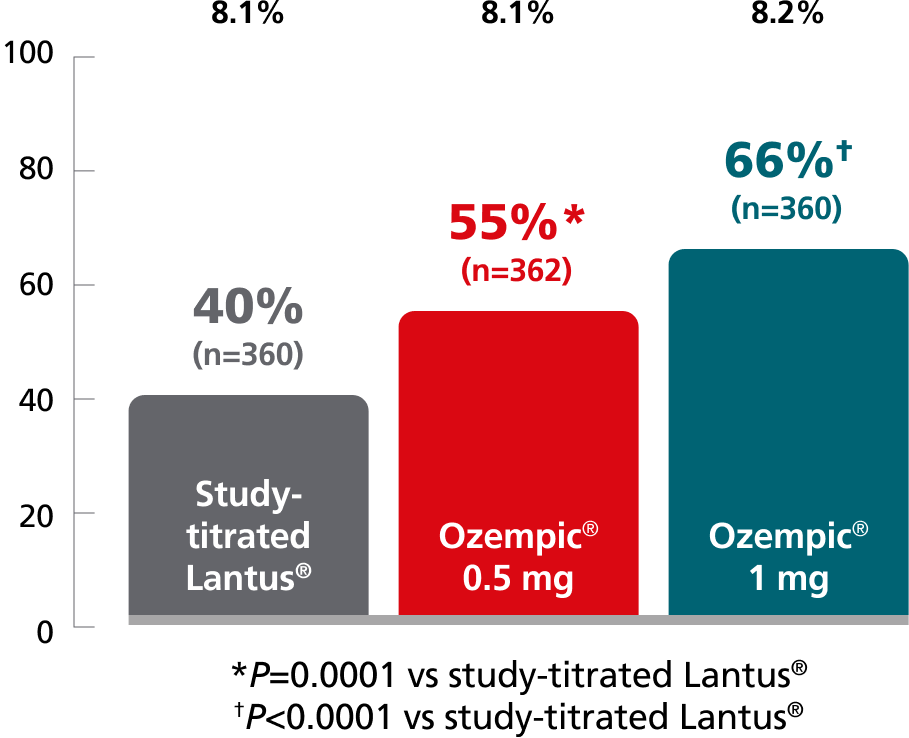
26% of insulin patients titrated to goal by Week 30.
Mean daily insulin dose: 29 U/day
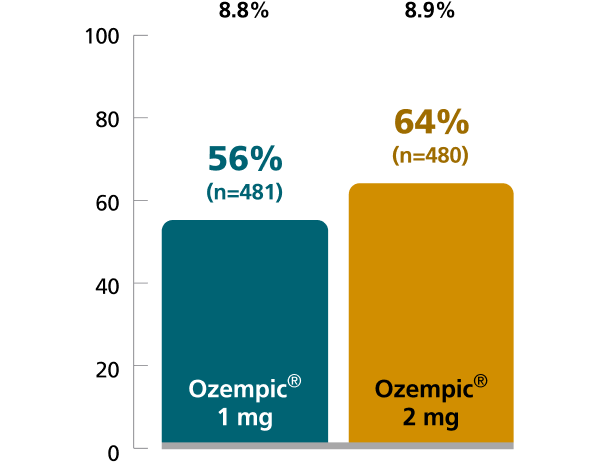
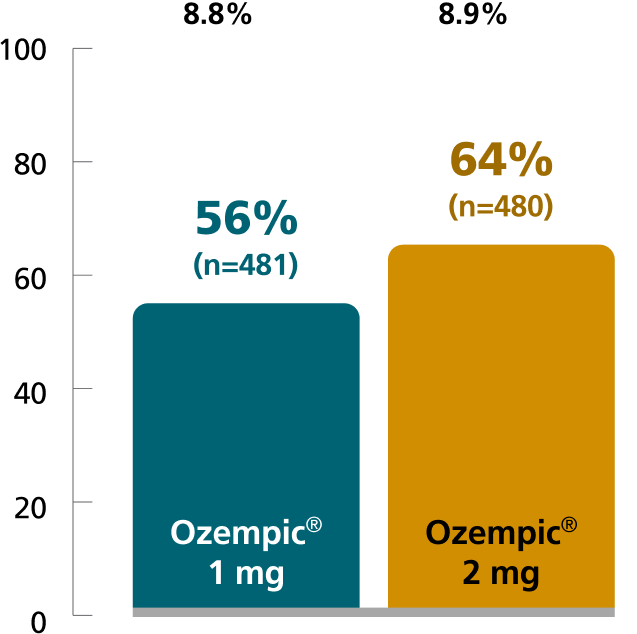
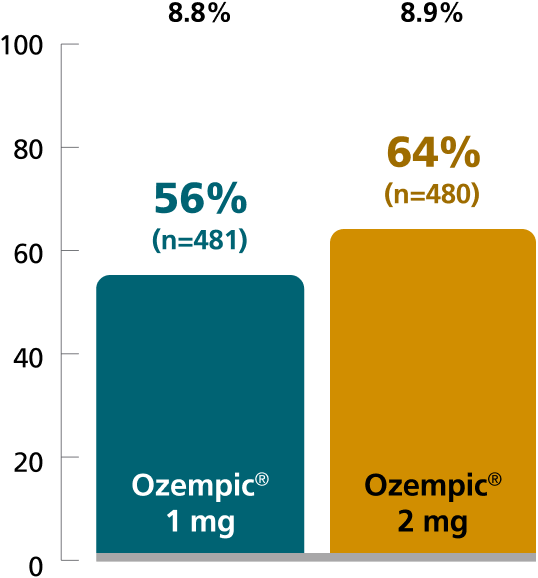
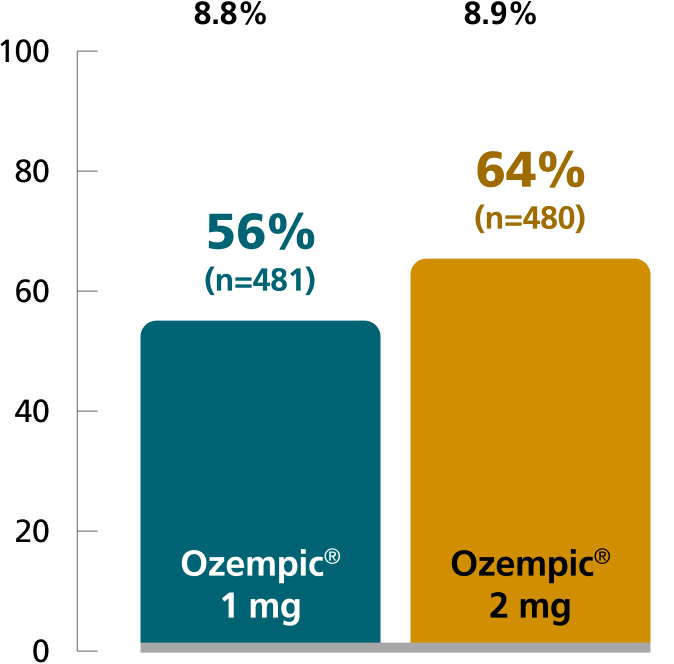
SUSTAIN FORTE:
Ozempic® 1 mg vs 2 mg1,4
In patients with type 2 diabetes on metformin ± sulfonylurea
Percent of patients who achieved A1C <7% at Week 40
Mean baseline A1C:
SUSTAIN 4: Predefined secondary endpoint based on a post hoc analysis of retrieved dropout population. Results are from a 30-week, randomized, open-label, active-controlled trial in 1089 insulin-naïve adult patients on metformin ± sulfonylurea with type 2 diabetes comparing Ozempic® injection 0.5 mg and Ozempic® injection 1 mg with Lantus®.1,9
SUSTAIN FORTE: Predefined secondary endpoint based on analysis of retrieved dropout population. Values are dichotomized and denominator is the number of all randomized subjects. Due to statistical hierarchy, differences were not formally tested. Results are from a 40-week, randomized, active-controlled trial in 961 adult patients with type 2 diabetes on metformin with or without a sulfonylurea, comparing Ozempic® injection 1 mg with Ozempic® injection 2 mg.1,4
aAccording to the ADA, an A1C goal of <7% is appropriate for many nonpregnant adults without severe hypoglycemia or hypoglycemia affecting health or quality of life. However, a prescriber may recommend a different goal based on age, other health conditions, and other factors.5
ADA=American Diabetes Association.
Ozempic® vs Lantus® and Ozempic® 1 mg vs 2 mg1
SUSTAIN 4:
vs study-titrated Lantus®1,9
In insulin-naïve adult patients with type 2 diabetes on metformin ± sulfonylurea
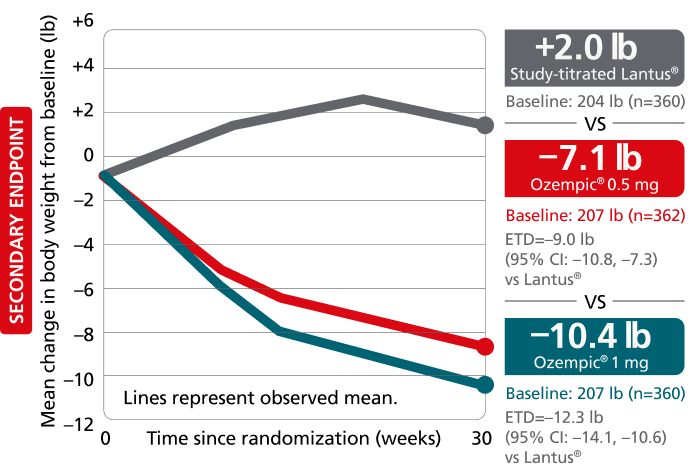
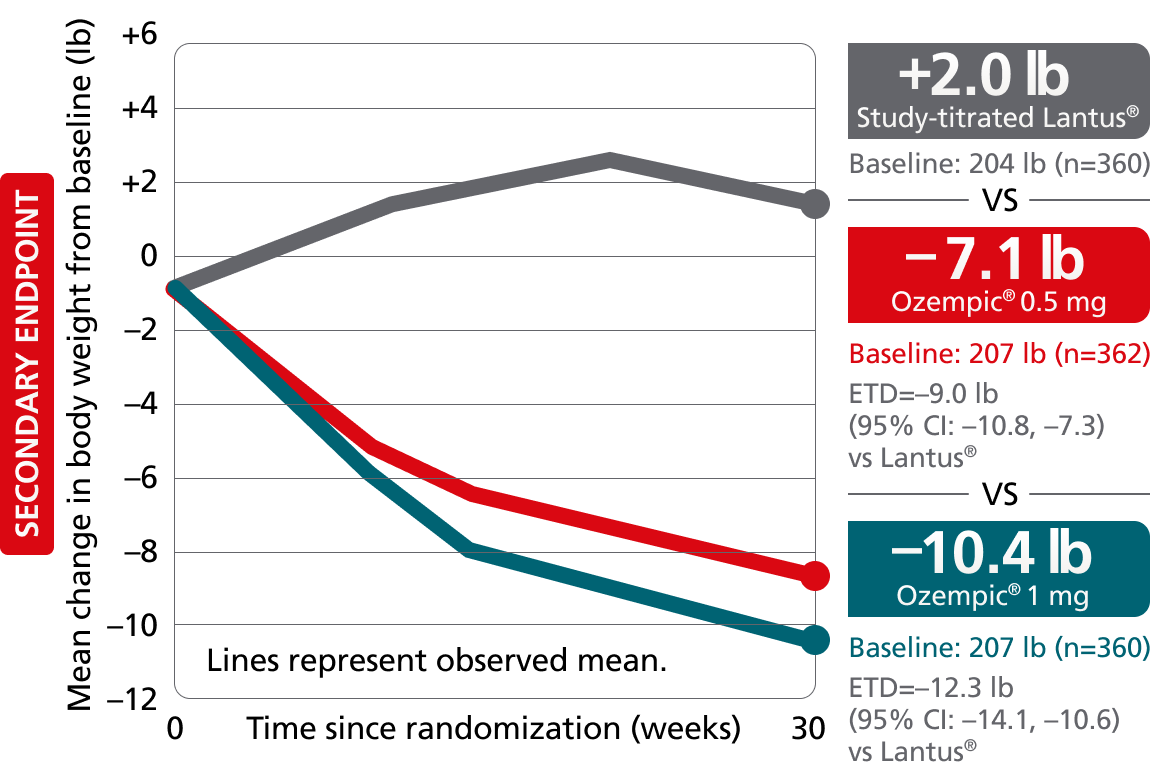
Secondary endpoint: mean change in body weight from baseline to Week 30
Mean baseline: 206 lb
SUSTAIN FORTE:
Ozempic® 1 mg vs 2 mg1,4,8
In adult patients with type 2 diabetes on metformin ± sulfonylurea
Secondary endpoint: mean change in body weight from baseline to Week 40
Mean baseline: 219 lb
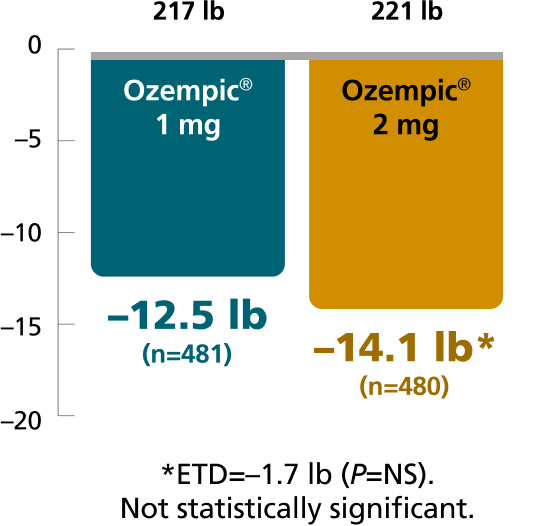
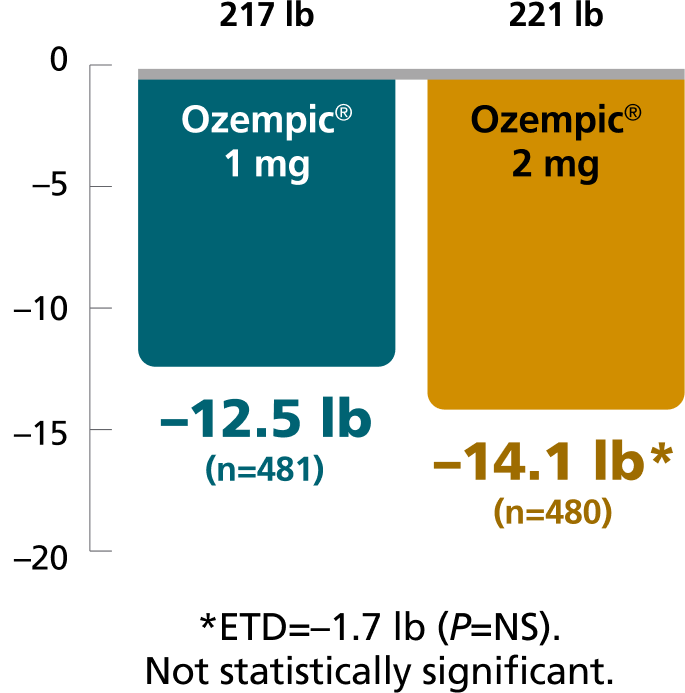
Results based on sensitivity analyses of retrieved dropout population. SUSTAIN 4 and SUSTAIN FORTE were only powered to detect differences in A1C from baseline to Week 30 and Week 40, respectively.
The estimated treatment difference was from baseline to Week 30 for SUSTAIN 4 and from baseline to Week 40 for SUSTAIN FORTE.
SUSTAIN 4: A 30-week, randomized, open-label, active-controlled trial in 1089 insulin-naïve adult patients on metformin ± sulfonylurea with type 2 diabetes comparing Ozempic® injection 0.5 mg and Ozempic® injection 1 mg with Lantus®.9
SUSTAIN FORTE: A 40-week, randomized, active-controlled trial in 961 adult patients with type 2 diabetes on metformin with or without a sulfonylurea, comparing Ozempic® injection 1 mg with Ozempic® injection 2 mg.1,4
Adverse events ≥5% in SUSTAIN 49
AEs occurring in ≥5% of participants treated with Ozempic® injection in SUSTAIN 4
SUSTAIN 4 was not designed to evaluate relative safety between Ozempic® injection and Lantus®

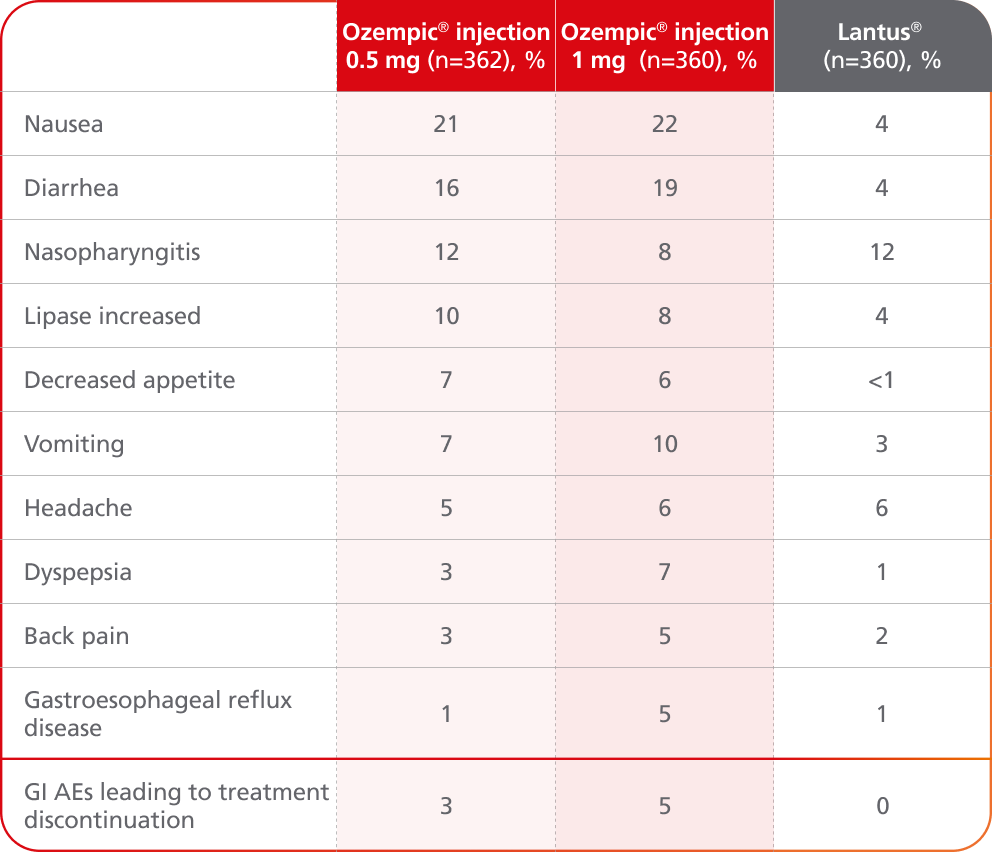
- In placebo-controlled trials, the most common adverse reactions reported in ≥5% of patients treated with Ozempic® injection are nausea, vomiting, diarrhea, abdominal pain, and constipation1
- Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared with rates in the clinical trials of another drug and may not reflect the rates observed in practice1
- Comparator AE rates are not an adequate basis for comparison of safety between products1
- Incidence of severe hypoglycemia was ≤1.5% across all placebo-controlled trials1
- Incidence of severe hypoglycemia or blood glucose-confirmed hypoglycemia (% of patients) was 4% with Ozempic® injection 0.5 mg, 6% with Ozempic® injection 1 mg, and 11% with Lantus®9,a
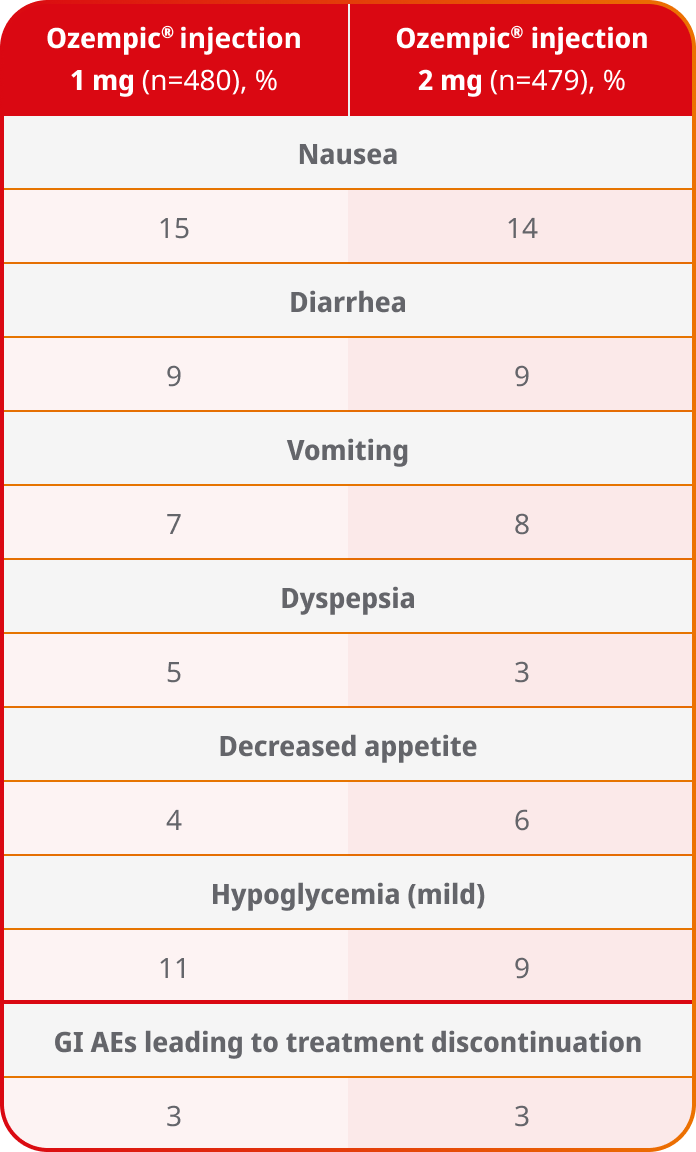
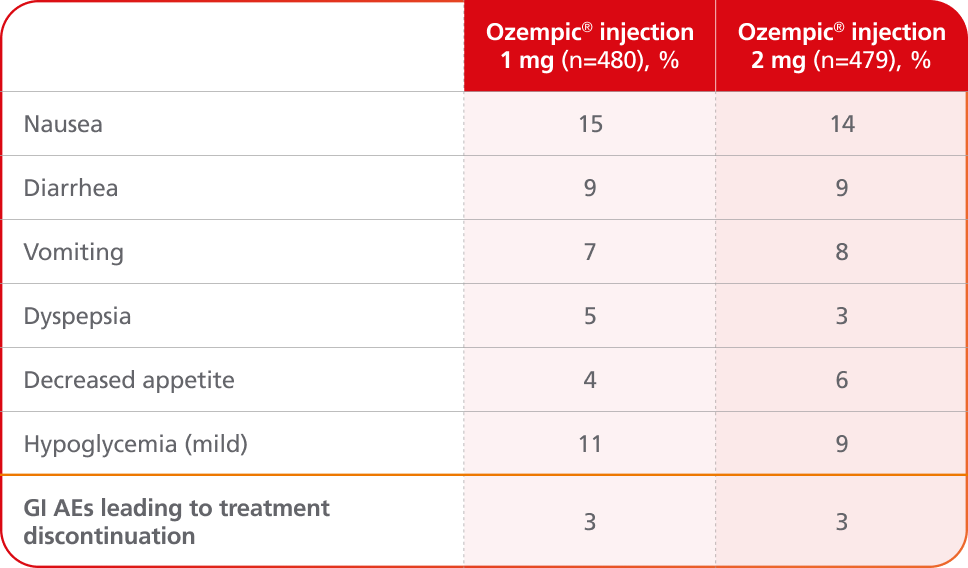
Adverse events ≥5% in SUSTAIN FORTE4
AEs occurring in ≥5% of patients receiving Ozempic® injection 1 mg and 2 mg in SUSTAIN FORTE
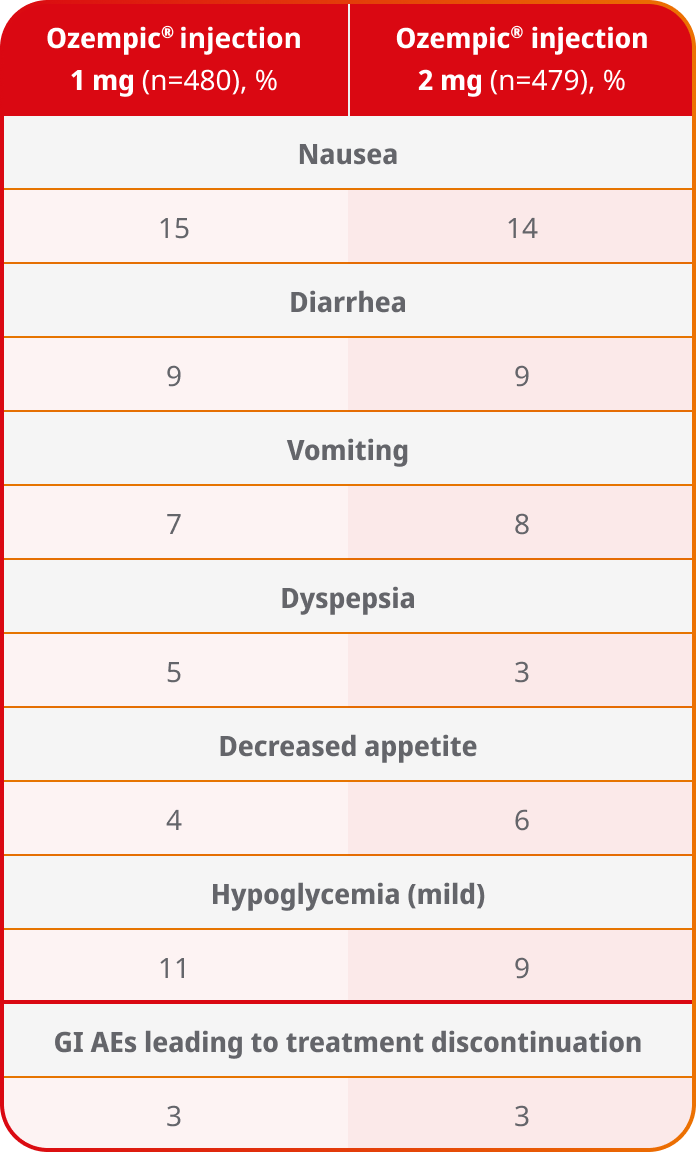
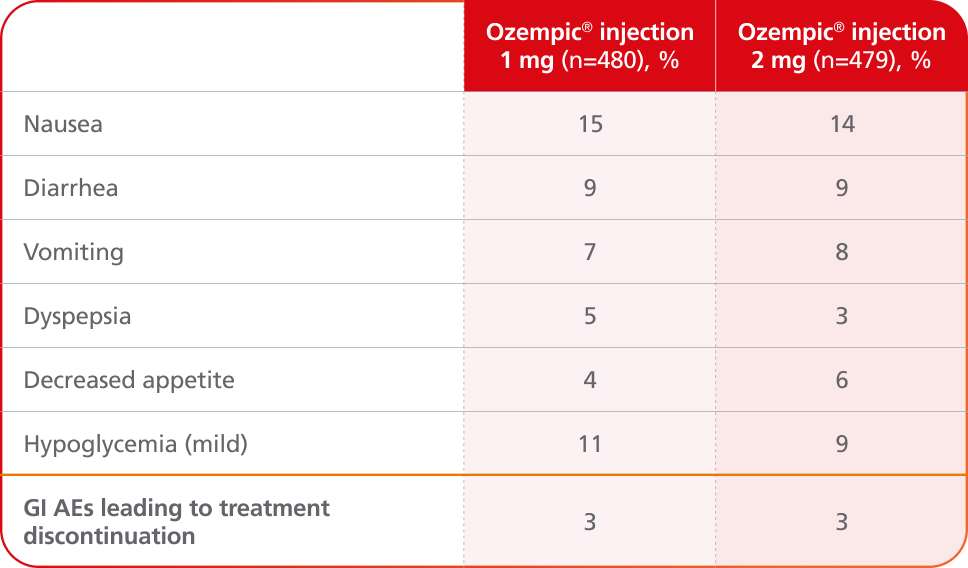
- In placebo-controlled trials, the most common adverse reactions reported in ≥5% of patients treated with Ozempic® injection are nausea, vomiting, diarrhea, abdominal pain, and constipation1
- No new safety signals were identified. Gastrointestinal adverse reactions occurred more frequently among patients receiving Ozempic® injection 2 mg (34.0%) vs Ozempic® injection 1 mg (30.8%)4
- Incidence of severe hypoglycemia (level 3) was <1% for Ozempic® injection 1 mg and Ozempic® injection 2 mg in the SUSTAIN FORTE trial4
aDefined as an event requiring assistance of another person to actively administer carbohydrates, glucagon, or take other corrective actions or blood glucose-confirmed symptomatic hypoglycemia (plasma glucose ≤3.1 mmol/L [56 mg/dL]).9
AE=adverse event; GI=gastrointestinal.
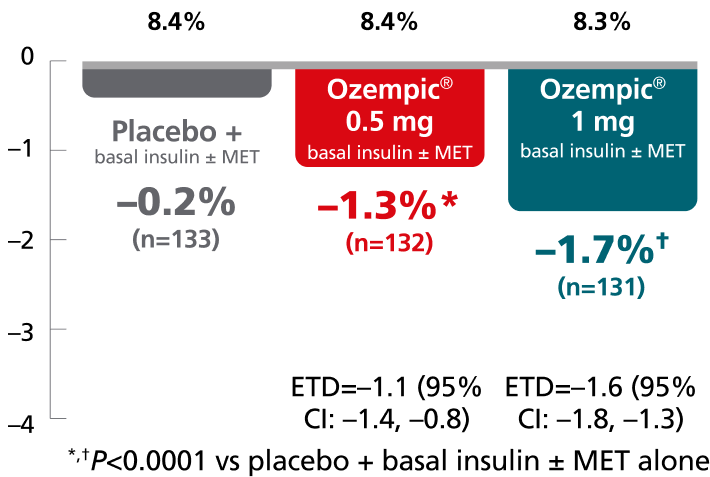
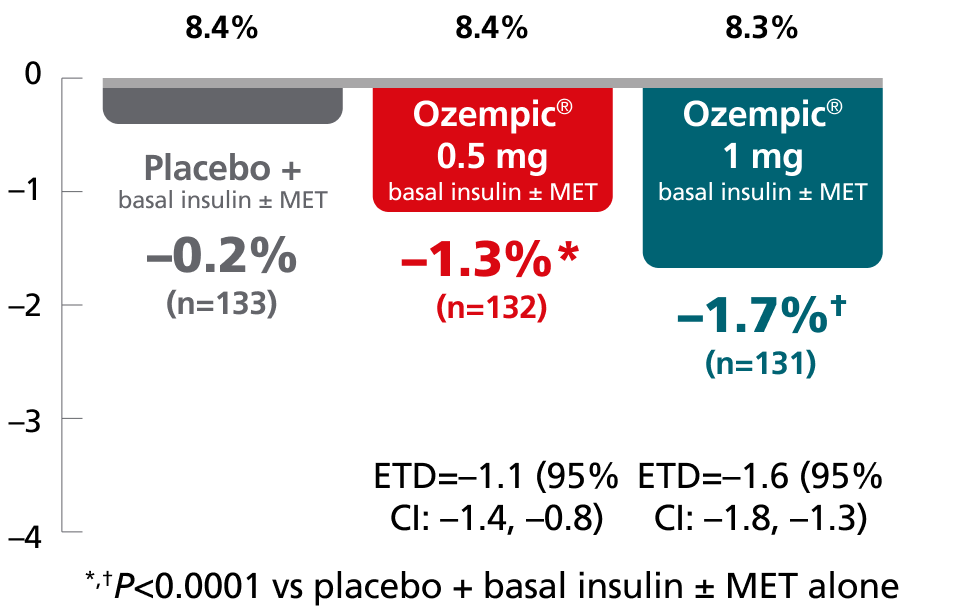
Ozempic® as an add-on to basal insulin and Ozempic® 1 mg vs 2 mg
Primary endpoint: change in A1C from baseline
SUSTAIN 5:
add-on basal insulin1,10,11
In adult patients with type 2 diabetes on basal insulin ± metformin
Mean change in A1C from baseline at Week 30
Mean baseline A1C:
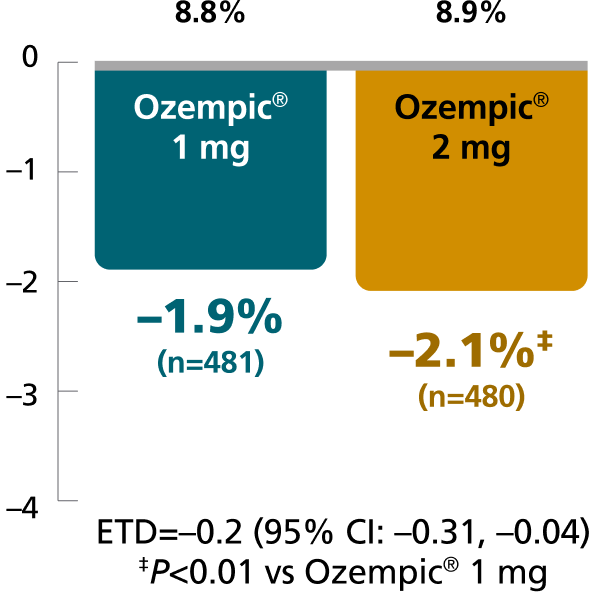
SUSTAIN FORTE:
Ozempic® 1 mg vs 2 mg1,8
In patients with type 2 diabetes on metformin ± sulfonylurea
Mean change in A1C from baseline at Week 40
Mean baseline A1C:
Results for SUSTAIN 5 and SUSTAIN FORTE based on sensitivity analyses of retrieved dropout population.
SUSTAIN 5: A 30-week, randomized, double-blind, placebo-controlled, parallel-group trial in 397 adult patients with type 2 diabetes evaluating the addition of Ozempic® injection 0.5 mg and Ozempic® injection 1 mg to basal insulin ± metformin. Patients with A1C ≤8% at screening had their background basal insulin dose reduced by 20% at the start of the trial to limit potential risk of hypoglycemia.1,10
SUSTAIN FORTE: A 40-week, randomized, active-controlled trial in 961 adult patients with type 2 diabetes on metformin with or without a sulfonylurea, comparing Ozempic® injection 1 mg with Ozempic® injection 2 mg.1,4
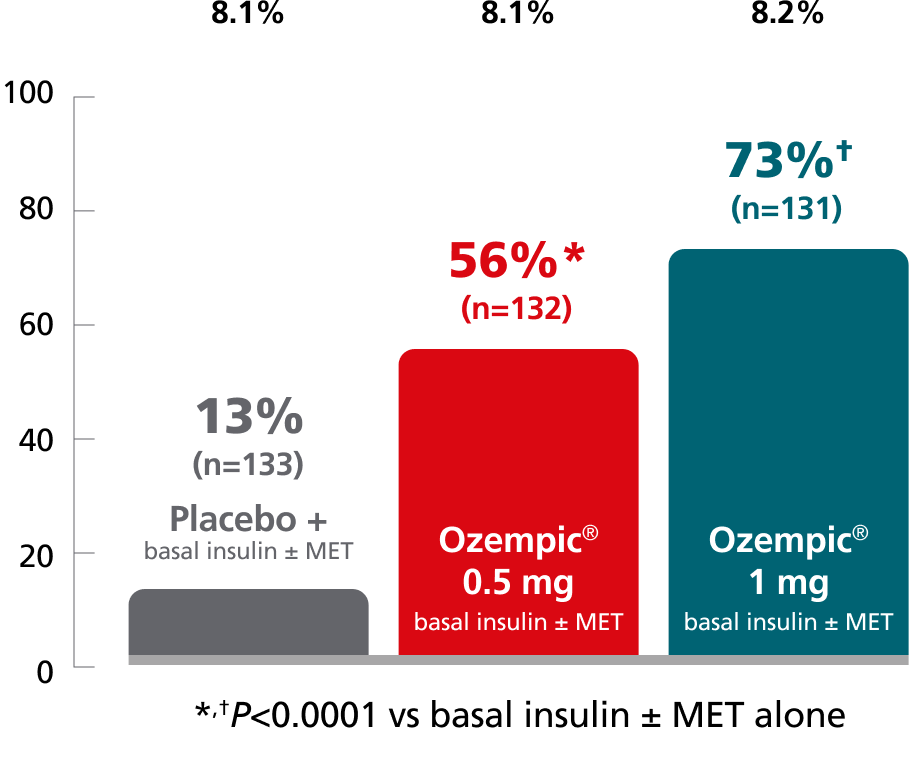
SUSTAIN 5:
add-on basal insulin1,10
In adult patients with type 2 diabetes on basal insulin ±
metformin
Mean change in A1C from baseline at Week 30
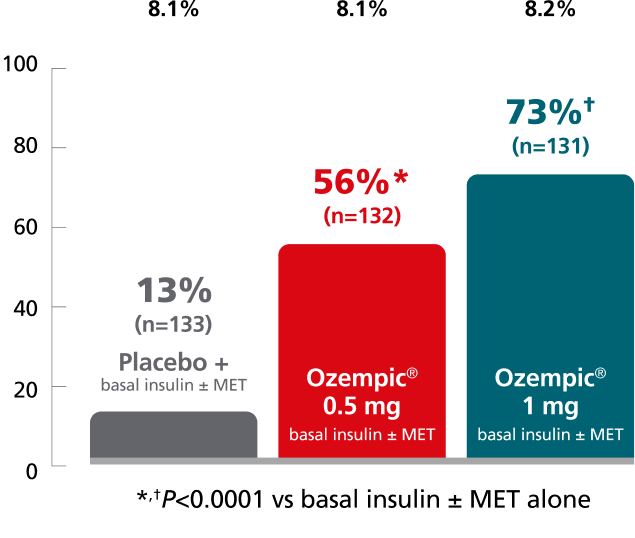
Patients with A1C ≤8% at screening had their background basal insulin dose reduced by 20% at the start of the trial to limit the potential risk of hypoglycemia.
SUSTAIN FORTE:
Ozempic® 1 mg vs 2 mg1,4
In patients with type 2 diabetes on metformin ± sulfonylurea
Mean change in A1C from baseline at Week 40
Patients achieving A1C <7% at Week 40 (%)
SUSTAIN 5: Predefined secondary endpoint analyzed using post hoc analysis of retrieved dropout population. Results are from a 30-week, randomized, double-blind, placebo-controlled, parallel-group trial in 397 adult patients with type 2 diabetes evaluating the addition of Ozempic® injection 0.5 mg and Ozempic® injection 1 mg to basal insulin ± metformin.1,10
SUSTAIN FORTE: Predefined secondary endpoint based on analysis of retrieved dropout population. Values are dichotomized and denominator is the number of all randomized subjects. Due to statistical hierarchy, differences were not formally tested. Results are from a 40-week, randomized, active-controlled trial in 961 adult patients with type 2 diabetes on metformin with or without a sulfonylurea, comparing Ozempic® injection 1 mg with Ozempic® injection 2 mg.1,4
aAccording to the ADA, an A1C goal of <7% is appropriate for many nonpregnant adults without severe hypoglycemia or hypoglycemia affecting health or quality of life. However, a prescriber may recommend a different goal based on age, other health conditions, and other factors.5
ADA=American Diabetes Association; AE=adverse event; CI=confidence interval; ETD=estimated treatment difference; GI=gastrointestinal; MET=metformin.
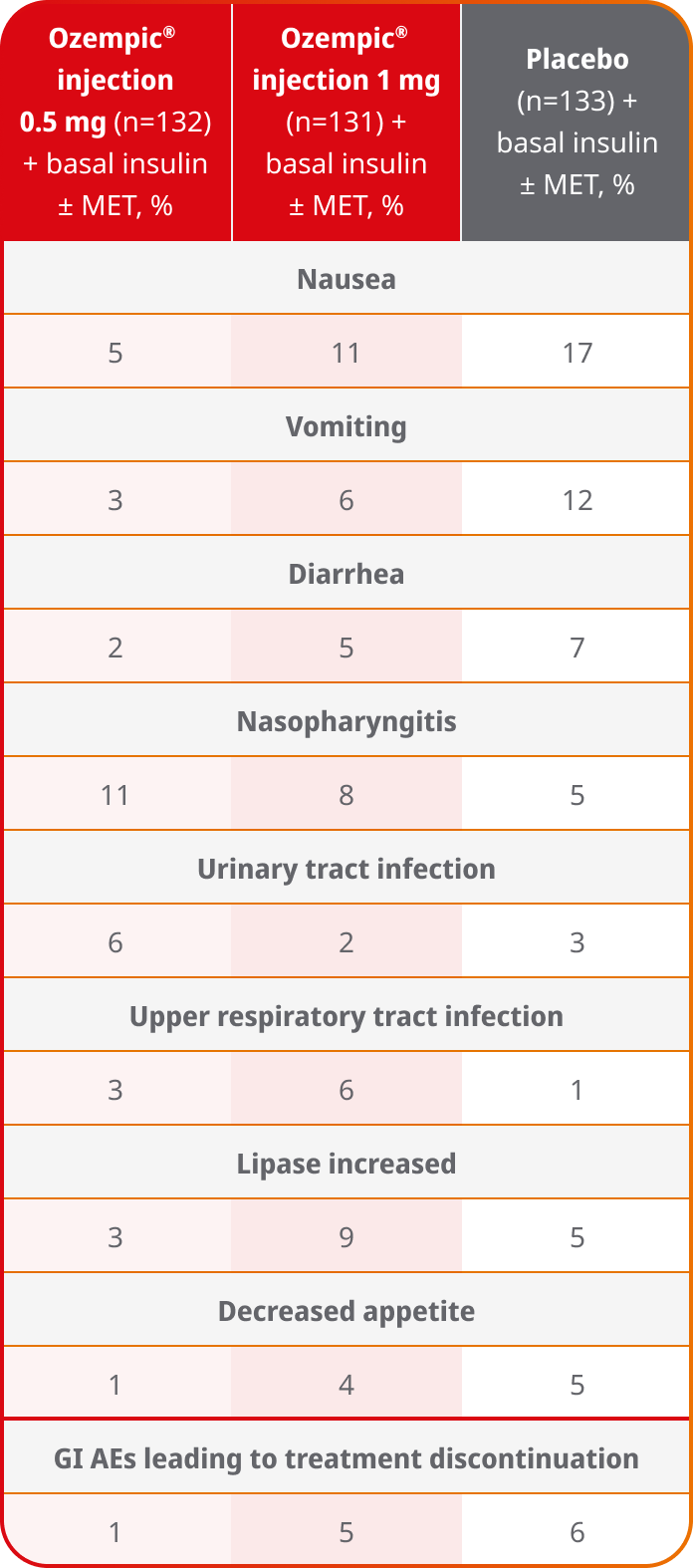
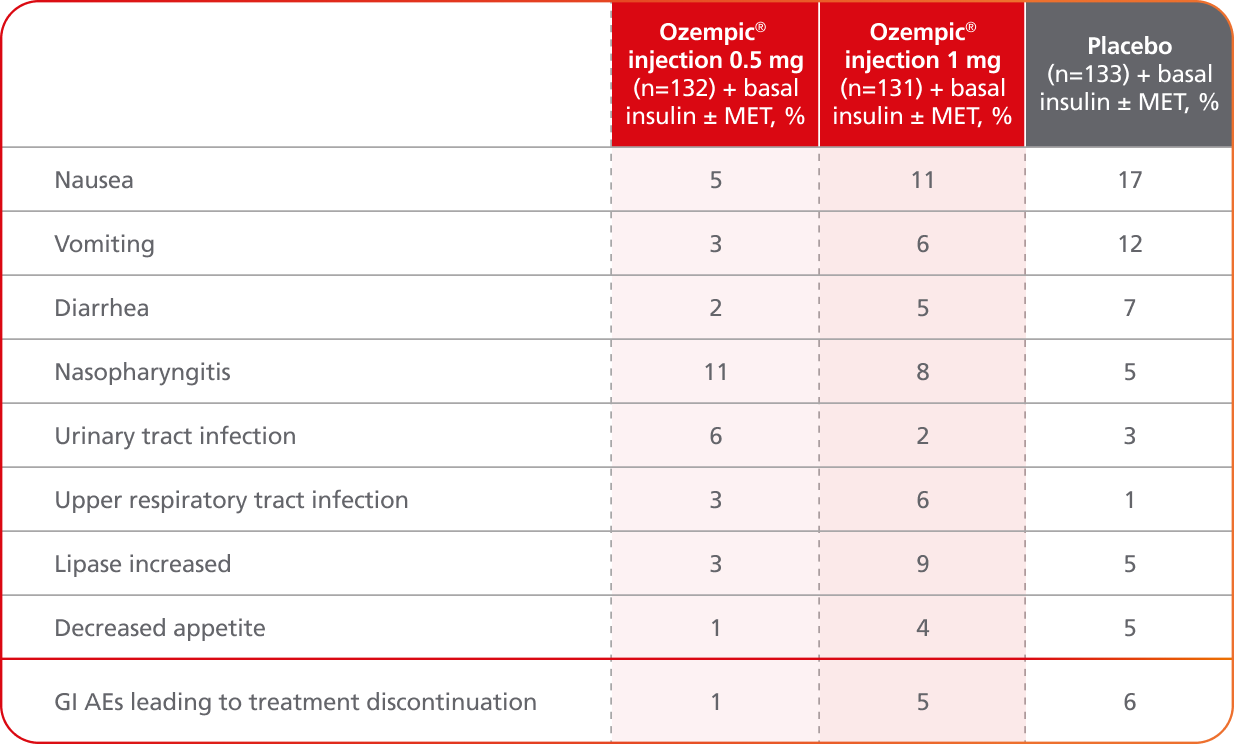
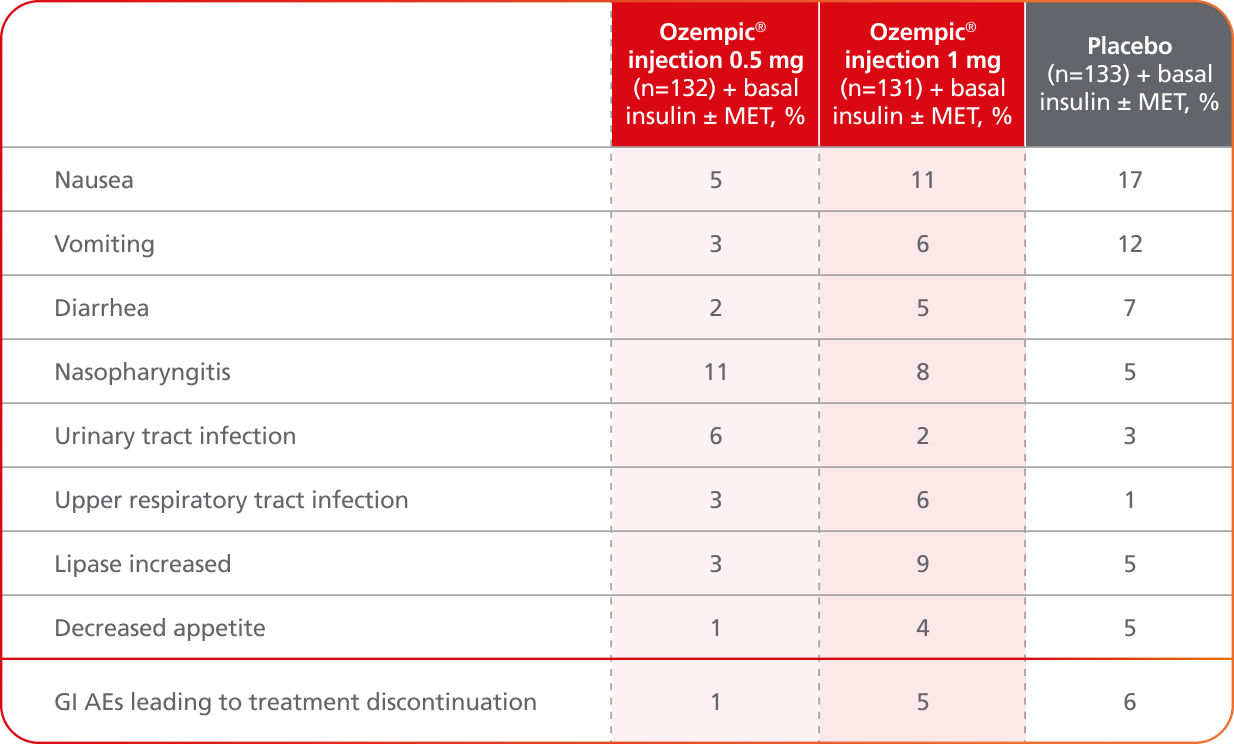
Adverse events ≥5% in SUSTAIN 58,10
AEs occurring in ≥5% of participants treated with Ozempic® injection in SUSTAIN 5
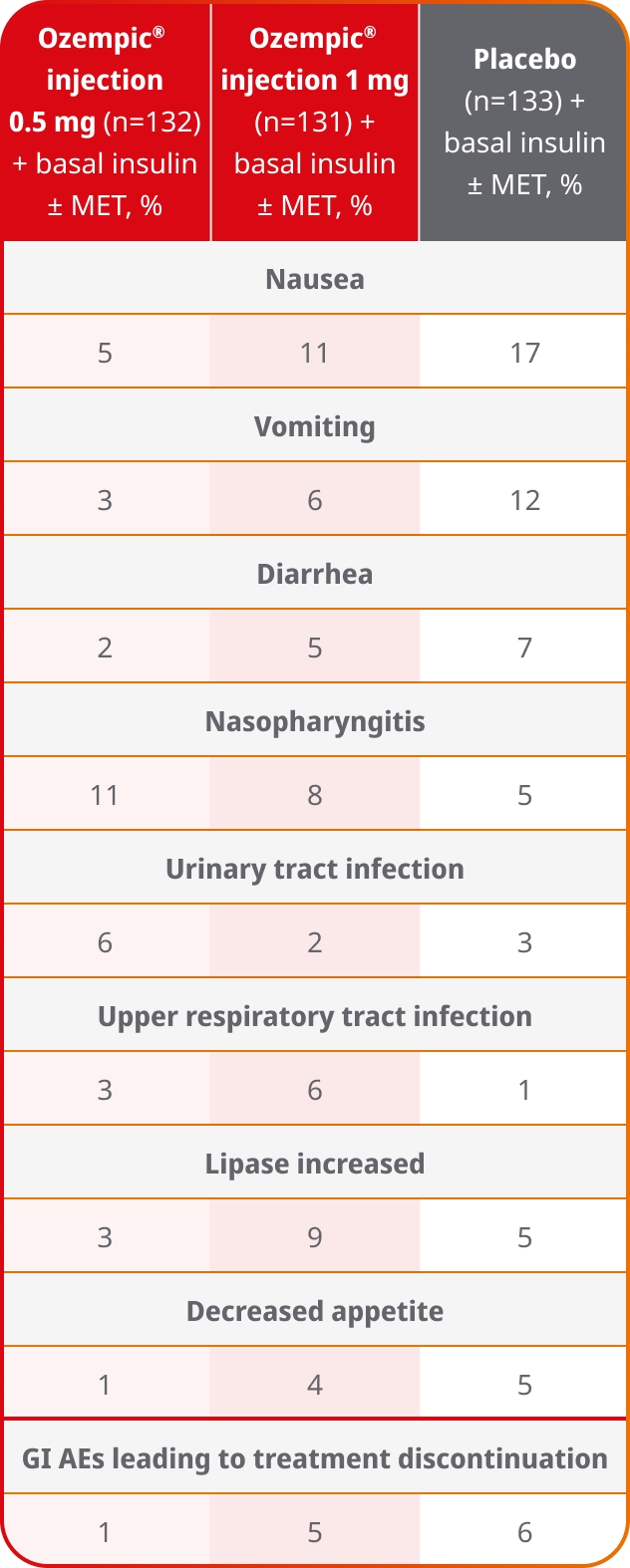
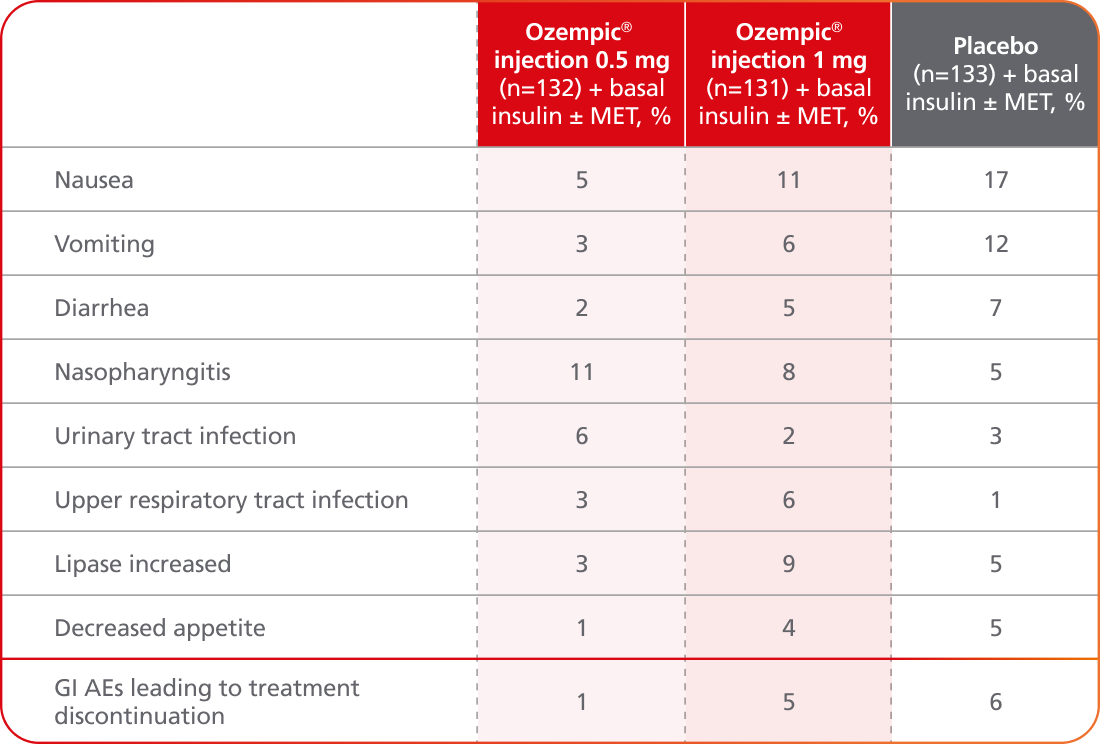
- Incidence of severe hypoglycemia was ≤1.5% across all placebo-controlled trials1
- Incidence of severe hypoglycemia or blood glucose-confirmed hypoglycemia (% of patients) was8,10:
- 8.3% with Ozempic® injection 0.5 mg + basal insulin ± MET
- 10.7% with Ozempic® injection 1 mg + basal insulin ± MET
- 5.3% with placebo + basal insulin ± MET
- Patients receiving Ozempic® injection in combination with an insulin secretagogue (eg, sulfonylurea) or insulin may have an increased risk of hypoglycemia, including severe hypoglycemia1
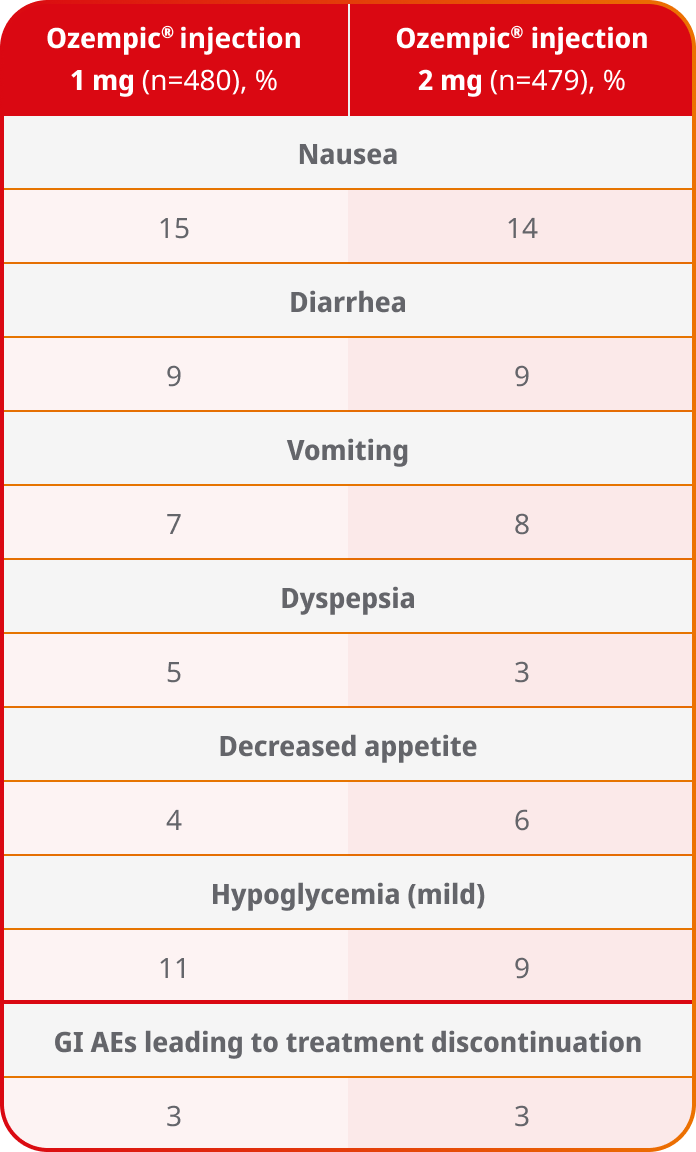
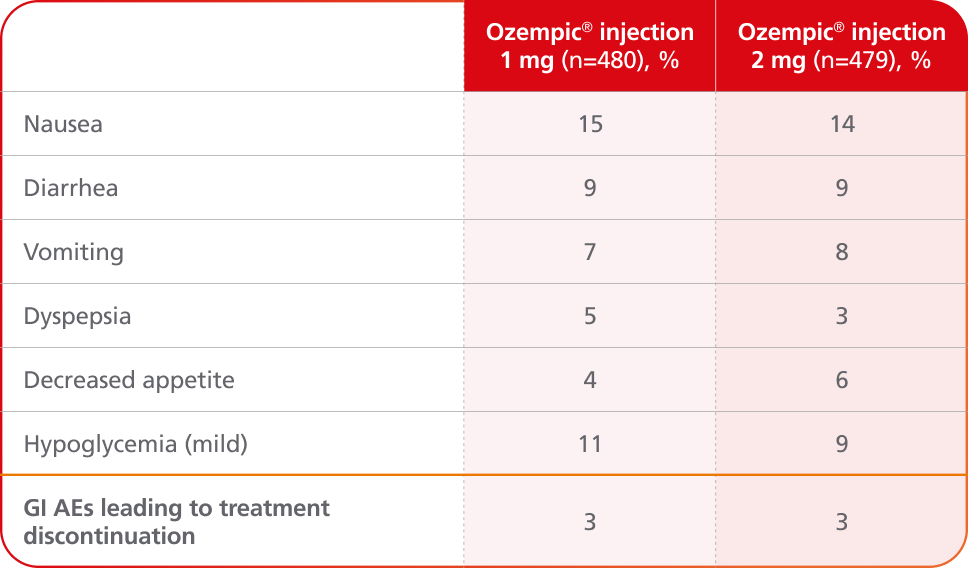
Adverse events ≥5% in SUSTAIN FORTE4
AEs occurring in ≥5% of patients receiving Ozempic® injection 1 mg and 2 mg in SUSTAIN FORTE
- In placebo-controlled trials, the most common adverse reactions reported in ≥5% of patients treated with Ozempic® injection are nausea, vomiting, diarrhea, abdominal pain, and constipation1
- No new safety signals were identified. Gastrointestinal adverse reactions occurred more frequently among patients receiving Ozempic® injection 2 mg (34.0%) vs Ozempic® injection 1 mg (30.8%)4
- Incidence of severe hypoglycemia (level 3) was <1% for Ozempic® injection 1 mg and Ozempic® injection 2 mg in the SUSTAIN FORTE trial4
SUSTAIN 5:
add-on basal insulin1,10
In adult patients with type 2 diabetes on basal insulin ±
metformin
Secondary endpoint: mean change in FPG at Week 30b
Baseline
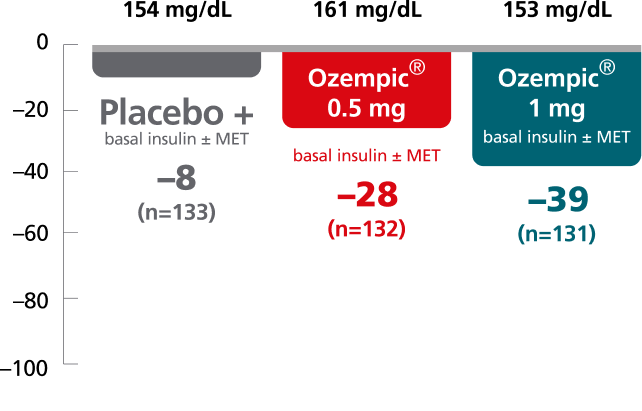
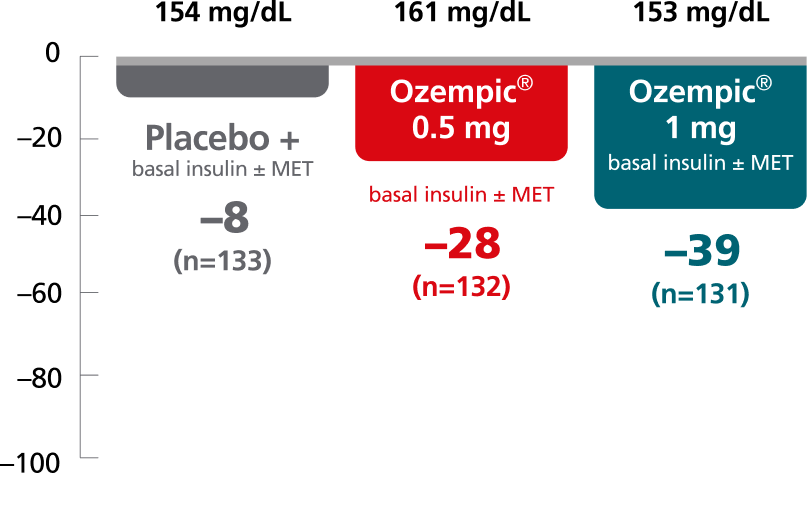
SUSTAIN 5:
add-on basal insulin8
In patients with type 2 diabetes on basal insulin ± metformin
Mean change in PPG at Week 30
Baseline

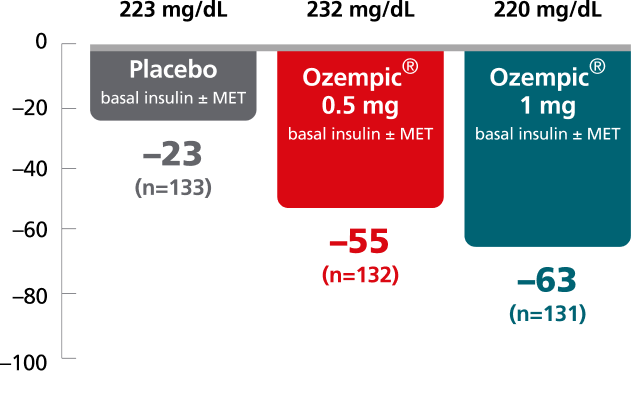
Mean change in 90-minute PPG from baseline at Week 30 was not a predefined endpoint. Post hoc analysis of absolute PPG was calculated from the 7-point SMPG profile.
The clinical relevance of FPG and PPG is unknown.
Patients with A1C ≤8% at screening had their background basal insulin dose reduced by 20% at the start of the trial to limit potential risk of hypoglycemia.10
Results are from a 30-week, randomized, double-blind, placebo-controlled, parallel-group trial in 397 adult patients with type 2 diabetes evaluating the addition of Ozempic® injection 0.5 mg and Ozempic® injection 1 mg to basal insulin ± metformin.10
bPredefined secondary endpoint using post hoc analysis of retrieved dropout population; not adjusted for multiplicity.10
Adverse events ≥5% in SUSTAIN 58,10
AEs occurring in ≥5% of participants treated with Ozempic® in SUSTAIN 5
- Incidence of severe hypoglycemia was ≤1.5% across all placebo-controlled trials1
- Incidence of severe hypoglycemia or blood glucose-confirmed hypoglycemia (% of patients) was8,10:
- 8.3% with Ozempic® 0.5 mg + basal insulin ± MET
- 10.7% with Ozempic® 1 mg + basal insulin ± MET
- 5.3% with placebo + basal insulin ± MET
- Patients receiving Ozempic® in combination with an insulin secretagogue (eg, sulfonylurea) or insulin may have an increased risk of hypoglycemia, including severe hypoglycemia1
ADA=American Diabetes Association; AE=adverse event; CI=confidence interval; ETD=estimated treatment difference; FPG=fasting plasma glucose; GI=gastrointestinal; MET=metformin; PPG=postprandial glucose; SMPG=self-monitoring of plasma glucose.
Ozempic® as an add-on to basal insulin and Ozempic® 1 mg vs 2 mg
SUSTAIN 5:
add-on basal insulin1,10
In patients with type 2 diabetes on basal insulin ± metformin
Secondary endpoint: mean change in body weight from baseline to Week 30
Mean baseline: 202 lb
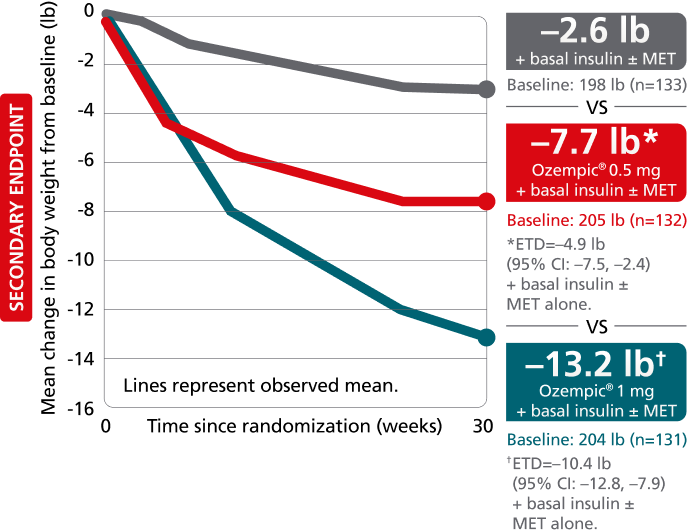
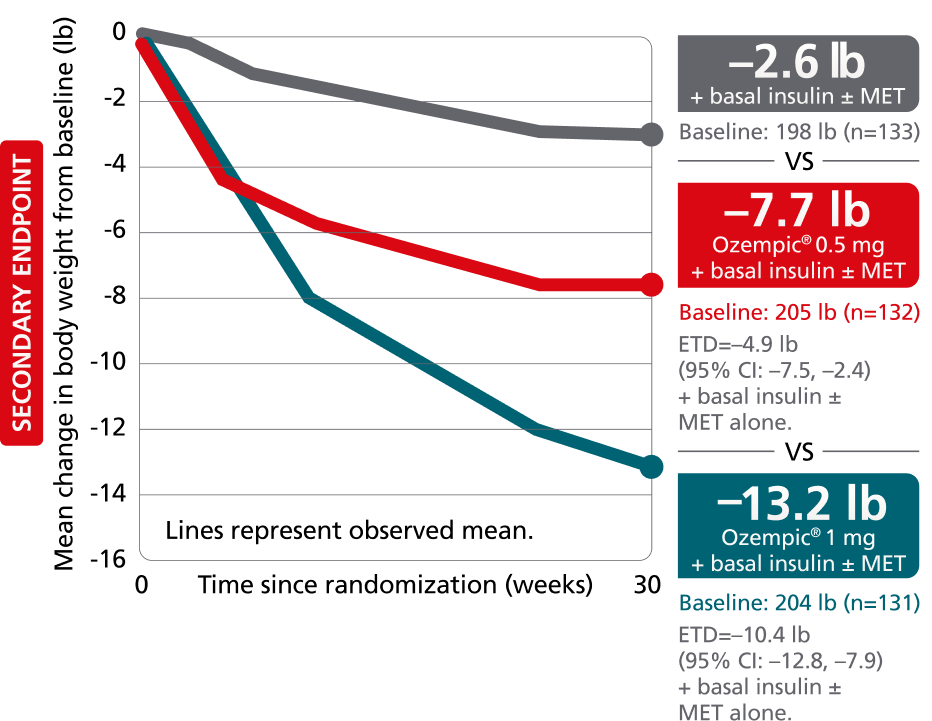
SUSTAIN FORTE:
Ozempic® 1 mg vs 2 mg1,4,8
In patients with type 2 diabetes on metformin ± sulfonylurea
Secondary endpoint: mean change in body weight from baseline to Week 40
Mean baseline: 219 lb
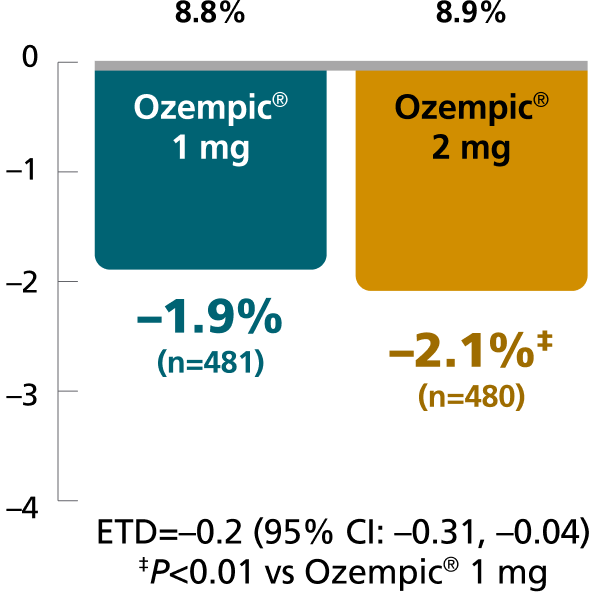
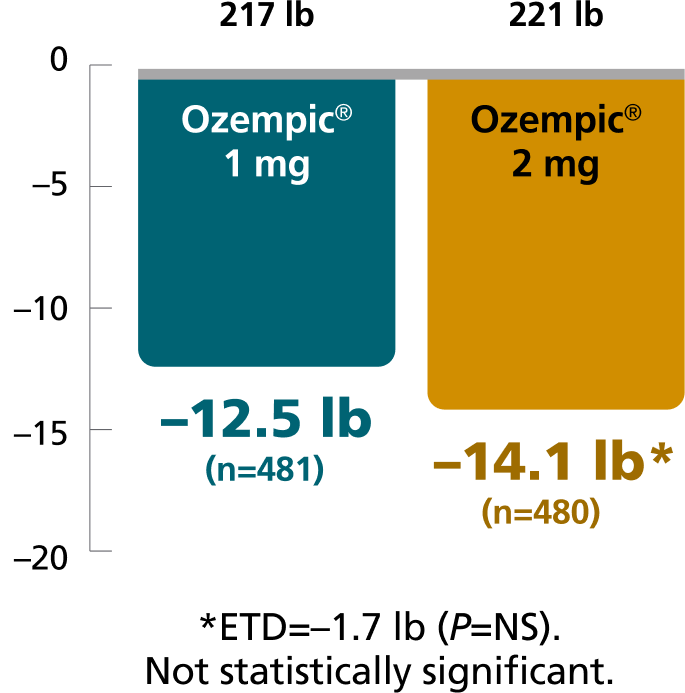
Results based on sensitivity analyses of retrieved dropout population. SUSTAIN 5 and SUSTAIN FORTE were only powered to detect differences in weight from baseline to Week 30 and Week 40, respectively.
The estimated treatment difference was from baseline to Week 30 for SUSTAIN 5 and from baseline to Week 40 for SUSTAIN FORTE.
SUSTAIN 5: A 30-week, randomized, double-blind, placebo-controlled, parallel-group trial in 397 adult patients with type 2 diabetes evaluating the addition of Ozempic® injection 0.5 mg and Ozempic® injection 1 mg to basal insulin ± metformin.1,10
SUSTAIN FORTE: A 40-week, randomized, active-controlled trial in 961 adult patients with type 2 diabetes on metformin with or without a sulfonylurea, comparing Ozempic® injection 1 mg with Ozempic® injection 2 mg.1,4
Adverse events ≥5% in SUSTAIN 58,10
AEs occurring in ≥5% of participants treated with Ozempic® injection in SUSTAIN 5
- Incidence of severe hypoglycemia was ≤1.5% across all placebo-controlled trials1
- Incidence of severe hypoglycemia or blood glucose-confirmed hypoglycemia (% of patients) was8,10:
- 8.3% with Ozempic® 0.5 mg + basal insulin ± MET
- 10.7% with Ozempic® 1 mg + basal insulin ± MET
- 5.3% with placebo + basal insulin ± MET
- Patients receiving Ozempic® injection in combination with an insulin secretagogue (eg, sulfonylurea) or insulin may have an increased risk of hypoglycemia, including severe hypoglycemia1
Adverse events ≥5% in SUSTAIN FORTE4
AEs occurring in ≥5% of patients receiving Ozempic® injection 1 mg and 2 mg in SUSTAIN FORTE
- In placebo-controlled trials, the most common adverse reactions reported in ≥5% of patients treated with Ozempic® injection are nausea, vomiting, diarrhea, abdominal pain, and constipation1
- No new safety signals were identified. Gastrointestinal adverse reactions occurred more frequently among patients receiving Ozempic® injection 2 mg (34.0%) vs Ozempic® injection 1 mg (30.8%)4
- Incidence of severe hypoglycemia (level 3) was <1% for Ozempic® injection 1 mg and Ozempic® injection 2 mg in the SUSTAIN FORTE trial4
AE=adverse event; Cl=confidence interval; ETD=estimated treatment difference; GI=gastrointestinal; MET=metformin; NS=not significant.
Could Ozempic® help your patients who have T2D and CVD?
More ways to help your patients with T2D
CV=cardiovascular; CVD=cardiovascular disease; MET=metformin; T2D=type 2 diabetes.
STUDY DESIGNS
SUSTAIN 4: Head-to-head vs Lantus® (insulin glargine U-100)1,9
Study design: 30-week, randomized, open-label, active-controlled, parallel-group, multinational, multicenter trial to evaluate the efficacy and safety of Ozempic® injection vs insulin glargine U-100.
Patients: A total of 1089 insulin-naïve adult patients with T2D inadequately controlled on metformin alone (48%) or in combination with sulfonylurea (51%) were randomized to receive once-weekly Ozempic® injection 0.5 mg (n=362), once-weekly Ozempic® injection 1 mg (n=360), or once-daily insulin glargine U-100 (n=360). Patients assigned to insulin glargine had a baseline mean A1C of 8.1% and were started on a dose of 10 units once daily. Insulin glargine dose adjustments occurred throughout the trial period based on self-measured fasting plasma glucose before breakfast, targeting 71 to <100 mg/dL. In addition, investigators could titrate insulin glargine based on their discretion between study visits. Twenty-six percent of patients had been titrated to goal by the primary endpoint at Week 30, at which time the mean daily insulin dose was 29 units per day.
Primary endpoint: Mean change in A1C from baseline at Week 30.
Secondary endpoints: Mean change in body weight from baseline at Week 30; proportion of patients achieving A1C <7% at Week 30.
SUSTAIN 5: As an add-on to basal insulin vs placebo1,10
Study design: 30-week, randomized, double-blind, placebo-controlled, parallel-group, multinational, multicenter trial to compare the efficacy and safety of Ozempic® injection in combination with basal insulin vs volume-matched placebo in combination with basal insulin.
Patients: A total of 397 adult patients with T2D inadequately controlled on basal insulin with or without metformin were randomized to once-weekly Ozempic® injection 0.5 mg (n=132), Ozempic® injection 1 mg (n=131), or placebo (n=133). Randomization was stratified according to A1C at screening. Patients with A1C ≤8% at screening reduced the insulin dose by 20% at the start of the trial to reduce the risk of hypoglycemia.
Primary endpoint: Mean change in A1C from baseline at Week 30.
Secondary endpoints: Mean change in body weight from baseline at Week 30; proportion of patients achieving A1C <7% at Week 30; change in mean fasting plasma glucose (FPG) at Week 30.
SUSTAIN FORTE: Ozempic® injection 1 mg vs 2 mg1,4
Study design: 40-week, randomized, active-controlled, parallel-group, double-blind, phase 3B efficacy and safety trial of Ozempic® injection 2 mg vs Ozempic® injection 1 mg in patients with T2D in need of treatment intensification.
Patients: A total of 961 adult patients with inadequately controlled T2D (A1C 8.0%-10.0%) on metformin with or without a sulfonylurea were randomized 1:1 to 2 mg (n=480) or 1 mg (n=481) of once-weekly Ozempic® injection.
Primary endpoint: Mean change in A1C from baseline at Week 40.
Secondary endpoints: Mean change in body weight from baseline at Week 40; proportion of patients achieving A1C <7% at Week 40.
SUSTAIN 9: Ozempic® injection as an add-on to SGLT-2i ± MET/SU6
Study design: 30-week, multinational, randomized, double-blind, parallel-group, placebo-controlled trial evaluating the efficacy and safety of adding Ozempic® injection 1 mg to SGLT-2i ± metformin/sulfonylurea vs SGLT-2i + placebo ± metformin/sulfonylurea. Patients were on SGLT-2i for an average of approximately 46 weeks at randomization.
Patients: A total of 302 adult patients with T2D inadequately controlled on SGLT-2i ± metformin/sulfonylurea were randomized to receive Ozempic® injection 1 mg (n=151) once weekly or volume-matched placebo (n=151) as an add-on to SGLT-2i ± metformin/sulfonylurea.
Primary endpoint: Mean change in A1C from baseline at Week 30.
Secondary endpoints: Mean change in body weight from baseline at Week 30; proportion of patients achieving A1C <7% at Week 30.
SGLT-2i=sodium-glucose co-transporter-2 inhibitor; SU=sulfonylurea.
Important Safety Information for Ozempic®
WARNING: RISK OF THYROID C-CELL TUMORS
- In rodents, semaglutide causes dose-dependent and treatment-duration- dependent thyroid C-cell tumors at clinically relevant exposures. It is unknown whether Ozempic® causes thyroid C-cell tumors, including medullary thyroid carcinoma (MTC), in humans as human relevance of semaglutide-induced rodent thyroid C-cell tumors has not been determined
- Ozempic® is contraindicated in patients with a personal or family history of MTC or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). Counsel patients regarding the potential risk for MTC with the use of Ozempic® and inform them of symptoms of thyroid tumors (e.g., a mass in the neck, dysphagia, dyspnea, persistent hoarseness). Routine monitoring of serum calcitonin or using thyroid ultrasound is of uncertain value for early detection of MTC in patients treated with Ozempic®
Contraindications
- Ozempic® is contraindicated in patients with a personal or family history of MTC or in patients with MEN 2, and in patients with a prior serious hypersensitivity reaction to semaglutide or to any of the excipients in Ozempic®. Serious hypersensitivity reactions including anaphylaxis and angioedema have been reported with Ozempic®
Warnings and Precautions
- Risk of Thyroid C-Cell Tumors: Patients should be further evaluated if serum calcitonin is measured and found to be elevated or thyroid nodules are noted on physical examination or neck imaging
- Acute Pancreatitis: Acute pancreatitis, including fatal and nonfatal hemorrhagic or necrotizing pancreatitis, has been observed in patients treated with GLP-1 receptor agonists, including semaglutide. Observe patients carefully for signs and symptoms of acute pancreatitis, which may include persistent or severe abdominal pain (sometimes radiating to the back), with or without nausea or vomiting. If pancreatitis is suspected, discontinue Ozempic® and initiate appropriate management
- Diabetic Retinopathy Complications: In a 2-year trial involving patients with type 2 diabetes and high cardiovascular risk, more events of diabetic retinopathy complications occurred in patients treated with Ozempic® injection (3%) compared to placebo (1.8%). In a pooled analysis of glycemic control trials, patients reported diabetic retinopathy related adverse reactions during the trial (4.2% with semaglutide tablets and 3.8% with comparator). The absolute risk increase for diabetic retinopathy complications was larger among patients with a history of diabetic retinopathy at baseline than among patients without a known history.
Rapid improvement in glucose control has been associated with a temporary worsening of diabetic retinopathy. Patients with a history of diabetic retinopathy should be monitored for progression of diabetic retinopathy - Never Share an Ozempic® Pen Between Patients: Ozempic® pens must never be shared between patients, even if the needle is changed. Pen-sharing poses a risk for transmission of blood-borne pathogens
- Hypoglycemia: Patients receiving Ozempic® in combination with an insulin secretagogue (e.g., sulfonylurea) or insulin may have an increased risk of hypoglycemia, including severe hypoglycemia. Inform patients using these concomitant medications of the risk of hypoglycemia and educate them on the signs and symptoms of hypoglycemia
- Acute Kidney Injury Due to Volume Depletion: There have been postmarketing reports of acute kidney injury, in some cases requiring hemodialysis, in patients treated with semaglutide. The majority of reported events occurred in patients who experienced gastrointestinal reactions leading to dehydration such as nausea, vomiting, or diarrhea. Monitor renal function in patients reporting adverse reactions to Ozempic® that could lead to volume depletion, especially during dosage initiation and escalation
- Severe Gastrointestinal (GI) Adverse Reactions: Use of Ozempic® has been associated with GI adverse reactions, sometimes severe. In clinical trials, severe GI adverse reactions were reported more frequently among patients who received Ozempic® injection (0.5 mg 0.4%, 1 mg 0.8%) than placebo (0%); and severe GI adverse reactions were reported more frequently among patients who received semaglutide tablets (7 mg 0.6%, 14 mg 2%) than placebo (0.3%). Severe GI adverse reactions have also been reported postmarketing with GLP-1 receptor agonists. Ozempic® is not recommended in patients with severe gastroparesis
- Hypersensitivity: Serious hypersensitivity reactions (e.g., anaphylaxis, angioedema) have been reported in patients treated with Ozempic®. If hypersensitivity reactions occur, discontinue use of Ozempic®; treat promptly per standard of care, and monitor until signs and symptoms resolve. Use caution in a patient with a history of angioedema or anaphylaxis with another GLP-1 receptor agonist
- Acute Gallbladder Disease: Acute events of gallbladder disease such as cholelithiasis or cholecystitis have been reported in GLP-1 receptor agonist trials and postmarketing. In placebo-controlled trials, cholelithiasis was reported in 1.5% and 0.4% of patients treated with Ozempic® injection 0.5 mg and 1 mg, respectively, and not reported in placebo-treated patients. In placebo-controlled trials to improve glycemic control, cholelithiasis was reported in 1% of patients treated with semaglutide tablets 7 mg. In a 4-year CV outcomes trial (Trial 7), cholelithiasis was reported in 1.1% of patients treated with semaglutide tablets 14 mg and in 0.9% of placebo-treated patients. In Trial 7, cholecystitis was reported in 1.1% treated with semaglutide tablets 14 mg and in 0.7% of placebo-treated patients. If cholelithiasis is suspected, gallbladder studies and appropriate clinical follow-up are indicated
- Pulmonary Aspiration During General Anesthesia or Deep Sedation: Ozempic® delays gastric emptying. There have been rare postmarketing reports of pulmonary aspiration in patients receiving GLP-1 receptor agonists undergoing elective surgeries or procedures requiring general anesthesia or deep sedation who had residual gastric contents despite reported adherence to preoperative fasting recommendations. Instruct patients to inform healthcare providers prior to any planned surgeries or procedures if they are taking Ozempic®
Adverse Reactions
- The most common adverse reactions reported in ≥5% of patients taking Ozempic® are nausea, vomiting, diarrhea, abdominal pain, and constipation. Decreased appetite was also reported in ≥5% of patients taking semaglutide tablets
Drug Interactions
- When initiating Ozempic®, consider reducing the dose of concomitantly administered insulin secretagogue (such as sulfonylureas) or insulin to reduce the risk of hypoglycemia
- Ozempic® causes a delay of gastric emptying and has the potential to impact the absorption of concomitantly administered oral medications. Monitor the effects of oral medications concomitantly administered with Ozempic®. Consider increased clinical or laboratory monitoring for medications that have a narrow therapeutic index or that require clinical monitoring
Use in Specific Populations
- Pregnancy: Available data with semaglutide use in pregnant women are not sufficient to determine a drug associated risk for major birth defects, miscarriage, or other adverse maternal or fetal outcomes. Discontinue Ozempic® in women at least 2 months before a planned pregnancy due to the long washout period for semaglutide
- Lactation: A clinical lactation study reported semaglutide concentrations below the lower limit of quantification in human breast milk. However, salcaprozate sodium (SNAC) and/or its metabolites are present in human milk. Because of the unknown potential for serious adverse reactions in the breastfed infant due to the possible accumulation of SNAC, an absorption enhancer for Ozempic® tablets, and because there are alternative formulations of semaglutide that do not contain SNAC that can be used during lactation, advise patients that breastfeeding is not recommended during treatment with Ozempic® tablets
Please click here for Ozempic® injection Prescribing Information, including Boxed Warning.
Please click here for Ozempic® tablets Prescribing Information, including Boxed Warning.
Indications and Usage
Ozempic® (semaglutide) injection 0.5 mg, 1 mg, or 2 mg and Ozempic® (semaglutide) tablets 4 mg or 9 mg are indicated:
- as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes
Ozempic® injection is indicated:
- to reduce the risk of major adverse cardiovascular (CV) events (CV death, nonfatal myocardial infarction, or nonfatal stroke) in adults with type 2 diabetes and established CV disease
- to reduce the risk of sustained eGFR decline, end-stage kidney disease, and cardiovascular death in adults with type 2 diabetes and chronic kidney disease
Ozempic® tablets are indicated:
- to reduce the risk of major adverse cardiovascular (CV) events (CV death, nonfatal myocardial infarction, or nonfatal stroke) in adults with type 2 diabetes who are at high risk for these events
Important Safety Information for Ozempic®
WARNING: RISK OF THYROID C-CELL TUMORS
- In rodents, semaglutide causes dose-dependent and treatment-duration- dependent thyroid C-cell tumors at clinically relevant exposures. It is unknown whether Ozempic® causes thyroid C-cell tumors, including medullary thyroid carcinoma (MTC), in humans as human relevance of semaglutide-induced rodent thyroid C-cell tumors has not been determined
- Ozempic® is contraindicated in patients with a personal or family history of MTC or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). Counsel patients regarding the potential risk for MTC with the use of Ozempic® and inform them of symptoms of thyroid tumors (e.g., a mass in the neck, dysphagia, dyspnea, persistent hoarseness). Routine monitoring of serum calcitonin or using thyroid ultrasound is of uncertain value for early detection of MTC in patients treated with Ozempic®
Important Safety Information for Ozempic®
WARNING: RISK OF THYROID C-CELL TUMORS
- In rodents, semaglutide causes dose-dependent and treatment-duration- dependent thyroid C-cell tumors at clinically relevant exposures. It is unknown whether Ozempic® causes thyroid C-cell tumors, including medullary thyroid carcinoma (MTC), in humans as human relevance of semaglutide-induced rodent thyroid C-cell tumors has not been determined
- Ozempic® is contraindicated in patients with a personal or family history of MTC or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). Counsel patients regarding the potential risk for MTC with the use of Ozempic® and inform them of symptoms of thyroid tumors (e.g., a mass in the neck, dysphagia, dyspnea, persistent hoarseness). Routine monitoring of serum calcitonin or using thyroid ultrasound is of uncertain value for early detection of MTC in patients treated with Ozempic®
Contraindications
- Ozempic® is contraindicated in patients with a personal or family history of MTC or in patients with MEN 2, and in patients with a prior serious hypersensitivity reaction to semaglutide or to any of the excipients in Ozempic®. Serious hypersensitivity reactions including anaphylaxis and angioedema have been reported with Ozempic®
Warnings and Precautions
- Risk of Thyroid C-Cell Tumors: Patients should be further evaluated if serum calcitonin is measured and found to be elevated or thyroid nodules are noted on physical examination or neck imaging
- Acute Pancreatitis: Acute pancreatitis, including fatal and nonfatal hemorrhagic or necrotizing pancreatitis, has been observed in patients treated with GLP-1 receptor agonists, including semaglutide. Observe patients carefully for signs and symptoms of acute pancreatitis, which may include persistent or severe abdominal pain (sometimes radiating to the back), with or without nausea or vomiting. If pancreatitis is suspected, discontinue Ozempic® and initiate appropriate management
- Diabetic Retinopathy Complications: In a 2-year trial involving patients with type 2 diabetes and high cardiovascular risk, more events of diabetic retinopathy complications occurred in patients treated with Ozempic® injection (3%) compared to placebo (1.8%). In a pooled analysis of glycemic control trials, patients reported diabetic retinopathy related adverse reactions during the trial (4.2% with semaglutide tablets and 3.8% with comparator). The absolute risk increase for diabetic retinopathy complications was larger among patients with a history of diabetic retinopathy at baseline than among patients without a known history.
Rapid improvement in glucose control has been associated with a temporary worsening of diabetic retinopathy. Patients with a history of diabetic retinopathy should be monitored for progression of diabetic retinopathy - Never Share an Ozempic® Pen Between Patients: Ozempic® pens must never be shared between patients, even if the needle is changed. Pen-sharing poses a risk for transmission of blood-borne pathogens
- Hypoglycemia: Patients receiving Ozempic® in combination with an insulin secretagogue (e.g., sulfonylurea) or insulin may have an increased risk of hypoglycemia, including severe hypoglycemia. Inform patients using these concomitant medications of the risk of hypoglycemia and educate them on the signs and symptoms of hypoglycemia
- Acute Kidney Injury Due to Volume Depletion: There have been postmarketing reports of acute kidney injury, in some cases requiring hemodialysis, in patients treated with semaglutide. The majority of reported events occurred in patients who experienced gastrointestinal reactions leading to dehydration such as nausea, vomiting, or diarrhea. Monitor renal function in patients reporting adverse reactions to Ozempic® that could lead to volume depletion, especially during dosage initiation and escalation
- Severe Gastrointestinal (GI) Adverse Reactions: Use of Ozempic® has been associated with GI adverse reactions, sometimes severe. In clinical trials, severe GI adverse reactions were reported more frequently among patients who received Ozempic® injection (0.5 mg 0.4%, 1 mg 0.8%) than placebo (0%); and severe GI adverse reactions were reported more frequently among patients who received semaglutide tablets (7 mg 0.6%, 14 mg 2%) than placebo (0.3%). Severe GI adverse reactions have also been reported postmarketing with GLP-1 receptor agonists. Ozempic® is not recommended in patients with severe gastroparesis
- Hypersensitivity: Serious hypersensitivity reactions (e.g., anaphylaxis, angioedema) have been reported in patients treated with Ozempic®. If hypersensitivity reactions occur, discontinue use of Ozempic®; treat promptly per standard of care, and monitor until signs and symptoms resolve. Use caution in a patient with a history of angioedema or anaphylaxis with another GLP-1 receptor agonist
- Acute Gallbladder Disease: Acute events of gallbladder disease such as cholelithiasis or cholecystitis have been reported in GLP-1 receptor agonist trials and postmarketing. In placebo-controlled trials, cholelithiasis was reported in 1.5% and 0.4% of patients treated with Ozempic® injection 0.5 mg and 1 mg, respectively, and not reported in placebo-treated patients. In placebo-controlled trials to improve glycemic control, cholelithiasis was reported in 1% of patients treated with semaglutide tablets 7 mg. In a 4-year CV outcomes trial (Trial 7), cholelithiasis was reported in 1.1% of patients treated with semaglutide tablets 14 mg and in 0.9% of placebo-treated patients. In Trial 7, cholecystitis was reported in 1.1% treated with semaglutide tablets 14 mg and in 0.7% of placebo-treated patients. If cholelithiasis is suspected, gallbladder studies and appropriate clinical follow-up are indicated
- Pulmonary Aspiration During General Anesthesia or Deep Sedation: Ozempic® delays gastric emptying. There have been rare postmarketing reports of pulmonary aspiration in patients receiving GLP-1 receptor agonists undergoing elective surgeries or procedures requiring general anesthesia or deep sedation who had residual gastric contents despite reported adherence to preoperative fasting recommendations. Instruct patients to inform healthcare providers prior to any planned surgeries or procedures if they are taking Ozempic®
Adverse Reactions
- The most common adverse reactions reported in ≥5% of patients taking Ozempic® are nausea, vomiting, diarrhea, abdominal pain, and constipation. Decreased appetite was also reported in ≥5% of patients taking semaglutide tablets
Drug Interactions
- When initiating Ozempic®, consider reducing the dose of concomitantly administered insulin secretagogue (such as sulfonylureas) or insulin to reduce the risk of hypoglycemia
- Ozempic® causes a delay of gastric emptying and has the potential to impact the absorption of concomitantly administered oral medications. Monitor the effects of oral medications concomitantly administered with Ozempic®. Consider increased clinical or laboratory monitoring for medications that have a narrow therapeutic index or that require clinical monitoring
Use in Specific Populations
- Pregnancy: Available data with semaglutide use in pregnant women are not sufficient to determine a drug associated risk for major birth defects, miscarriage, or other adverse maternal or fetal outcomes. Discontinue Ozempic® in women at least 2 months before a planned pregnancy due to the long washout period for semaglutide
- Lactation: A clinical lactation study reported semaglutide concentrations below the lower limit of quantification in human breast milk. However, salcaprozate sodium (SNAC) and/or its metabolites are present in human milk. Because of the unknown potential for serious adverse reactions in the breastfed infant due to the possible accumulation of SNAC, an absorption enhancer for Ozempic® tablets, and because there are alternative formulations of semaglutide that do not contain SNAC that can be used during lactation, advise patients that breastfeeding is not recommended during treatment with Ozempic® tablets
Please click here for Ozempic® injection Prescribing Information, including Boxed Warning.
Please click here for Ozempic® tablets Prescribing Information, including Boxed Warning.
Indications and Usage
Ozempic® (semaglutide) injection 0.5 mg, 1 mg, or 2 mg and Ozempic® (semaglutide) tablets 4 mg or 9 mg are indicated:
- as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes
Ozempic® injection is indicated:
- to reduce the risk of major adverse cardiovascular (CV) events (CV death, nonfatal myocardial infarction, or nonfatal stroke) in adults with type 2 diabetes and established CV disease
- to reduce the risk of sustained eGFR decline, end-stage kidney disease, and cardiovascular death in adults with type 2 diabetes and chronic kidney disease
Ozempic® tablets are indicated:
- to reduce the risk of major adverse cardiovascular (CV) events (CV death, nonfatal myocardial infarction, or nonfatal stroke) in adults with type 2 diabetes who are at high risk for these events
References:
- Ozempic injection. Prescribing information. Novo Nordisk Inc.
- Reserved
- Reserved
- Frías JP, Auerbach P, Bajaj HS, et al. Efficacy and safety of once-weekly semaglutide 2.0 mg versus 1.0 mg in patients with type 2 diabetes (SUSTAIN FORTE): a double-blind, randomised, phase 3B trial. Lancet Diabetes Endocrinol. 2021;9(9):563-574. doi:10.1016/S2213-8587(21)00174-1
- American Diabetes Association Professional Practice Committee. Older adults: standards of care in diabetes—2026. Diabetes Care. 2026;49(suppl 1): S277-S296. doi:10.2337/dc26-S013
- Zinman B, Bhosekar V, Busch R, et al. Semaglutide once weekly as add-on to SGLT-2 inhibitor therapy in type 2 diabetes (SUSTAIN 9): a randomised, placebo-controlled trial. Lancet Diabetes Endocrinol. 2019;7(5):356-367. doi:10.1016/S2213-8587(19)30066-X
- Zinman B, Bhosekar V, Busch R, et al. Semaglutide once weekly as add-on to SGLT-2 inhibitor therapy in type 2 diabetes (SUSTAIN 9): a randomised, placebo-controlled trial. Supplementary appendix. Lancet Diabetes Endocrinol. 2019;7(5):356-367. doi:10.1016/S2213-8587(19)30066-X
- Data on file. Novo Nordisk Inc; Plainsboro, NJ.
- Aroda VR, Bain SC, Cariou B, et al. Efficacy and safety of once-weekly semaglutide versus once-daily insulin glargine as add-on to metformin (with or without sulfonylureas) in insulin-naïve patients with type 2 diabetes (SUSTAIN 4): a randomized, open-label, parallel-group, multicentre, multinational, phase 3a trial. Lancet Diabetes Endocrinol. 2017:5(5):355-366. doi:10.1016/S2213-8587(17)30085-2
- Rodbard HW, Lingvay I, Reed J, et al. Semaglutide added to basal insulin in type 2 diabetes (SUSTAIN 5): a randomized, controlled trial. J Clin Endocrinol Metab. 2018;103(6):2291-2301. doi:10.1210/jc.2018-00070
- Rodbard HW, Lingvay I, Reed J, et al. Semaglutide added to basal insulin in type 2 diabetes (SUSTAIN 5): a randomized, controlled trial. Supplementary appendix. J Clin Endocrinol Metab. 2018;103(6):2291-2301. doi:10.1210/jc.2018-00070