
In combination with a reduced calorie diet and increased physical activity, Wegovy® injection is indicated for the treatment of noncirrhotic metabolic dysfunction-associated steatohepatitis (MASH), formerly known as nonalcoholic steatohepatitis (NASH), with moderate to advanced liver fibrosis (consistent with stages F2 to F3 fibrosis) in adults. Click for Limitations of Use.
The indication for MASH is approved under accelerated approval based on improvement of MASH and fibrosis. Continued approval for this indication may be contingent upon the verification and description of clinical benefit in a confirmatory trial.

Intended for payer, formulary committee, or other similar entity with knowledge and expertise in the area of healthcare economic analysis carrying out its responsibilities for the selection of drugs for coverage or reimbursement on behalf of healthcare organizations.
A highly prevalent, underdiagnosed disease driving clinical and economic burden2,3
MASH is a progressive liver disease linked to metabolic syndrome and can advance to fibrosis, cirrhosis, and other severe complications4
MASH is a progressive, potentially fatal liver disease that is on the rise and projected to affect
27 million
people in the US by 20305*
Suspect MASH in people with cardiometabolic conditions6
~1/3
of patients worldwide with obesity are also living with MASH7
~1/3
of patients worldwide with type 2 diabetes are also living with MASH8
MASH is a growing epidemic in the United States, affecting more than 6% of adults9†
- Despite its prevalence, fewer than 1% of adults receive a formal diagnosis3‡
- Undiagnosed MASH leaves people at risk for undetected fibrosis progression4
Most people with MASH remain undiagnosed—allowing silent, undetected fibrosis progression.4
*Projection is based on a Markov model.5
†Based on a back-calculation approach utilizing published estimates of average MASH-related cirrhosis prevalence and literature-derived proportions of cirrhosis among patients with MASH. Proportions of cirrhosis in patients with MASH were updated to 2020 country-specific obesity and type 2 diabetes prevalence.9
‡Based on real-world data from a large managed-care population from 2016 to 2020, this observational study employs longitudinal medical and pharmacy claims (ICD-10) data to identify patients with MASLD/MASH and calculate prevalence rates.3
ICD-10, International Classification of Diseases, Tenth Revision; MASLD, metabolic dysfunction-associated steatotic liver disease.
Rising clinical and economic burden2
In the United States, MASH is the leading cause of liver transplantation in women and adults >65 years10
Total estimated US liver transplant-related costs were over $11.1 billion in 202511§
Patients with MASLD/MASH with F3 fibrosis have high healthcare utilization with annual average costs of $30,000 per patient12¶
Patients with MASH and high FIB-4 scores experience 2x higher CV-related and ~34x higher liver-related medical costs vs patients with low FIB-4 scores3#
MASH with fibrosis increases clinical risk and drives higher healthcare costs.12,13
§Based on the Milliman 2025 report of estimated billed charges for organ and tissue transplants. Total annual costs were calculated using estimated billed charges across transplant-related care (30 days pretransplant through 180 days posttransplant, including procurement, hospital admission, physician services, and immunosuppression) and the estimated number of liver transplants in 2025 (10,916).11
¶Based on data from a retrospective cohort study of United States commercial health plan members aged ≥18 years with ≥1 non-diagnostic medical claim including a primary or secondary diagnosis code for MASLD and/or MASH between January 1, 2008, and August 31, 2016. The pre-index period was defined as the 6 months before the index date (first valid FIB-4 score), and the post-index period was defined as the earliest of 6 months, progression to advanced liver diseases, end of coverage, or end of the study period (post-index period). Fibrosis was identified by FIB-4 (n=3251).12
#Based on a retrospective cohort analysis of US adults with MASH using administrative claims from the Healthcare Integrated Research Database (HIRD). Patients were stratified by Fibrosis 4 (FIB 4) score into low, indeterminate, and high categories. Post-index cardiovascular-related and liver-related medical costs were compared across FIB 4 strata using generalized linear regression models adjusted for demographic, clinical, and comorbidity index factors.3
CV, cardiovascular; FIB-4, fibrosis-4.
Guidance recommends early and targeted screening (identification)14
Professional society guidance (eg, AASLD, AACE, ADA, and AGA) recommends screening for advanced fibrosis in high-risk populations, particularly those with metabolic risk factors6,14-16
- More than 2 in 5 patients with MASLD have metabolic syndrome17
Noninvasive tests (NITs) are recommended to support fibrosis risk stratification4
Cardiometabolic conditions associated with increased risk of MASH and fibrosis6,14
Fatty liver or family
history of cirrhosis
Type 2 diabetes
or prediabetes
Obesity
Hypertension
High triglycerides
Low HDL
Persistently elevated liver enzymes
(over 6 months)
PCOS
(polycystic ovary syndrome)
Early identification and management of MASH is critical18
AACE, American Association of Clinical Endocrinology; AASLD, American Association for the Study of Liver Diseases; ADA, American Diabetes Association; AGA, American Gastroenterological Association; HDL, high-density lipoprotein.
ESSENCE: A 240-week, 2-part, double-blind, placebo-controlled, phase 3 trial that randomized 1,197 adults with noncirrhotic MASH with fibrosis stage 2 or 3 and NAS ≥4 (≥1 in steatosis, lobular inflammation, and hepatocyte ballooning).1,19 1,195 patients were exposed to treatment and were included in the safety population.1 The efficacy of Wegovy® on liver histology was assessed in a Week 72 analysis using post-baseline biopsies from the first 800 patients (with F2 or F3 at eligibility), who were randomized 1:2 to receive placebo (n=266) or Wegovy® once weekly (n=534), in addition to standard of care for cardiometabolic comorbidities and healthy lifestyle counseling.1‖ Wegovy® or matching placebo was escalated to 2.4 mg once weekly during the initial 16 weeks of the treatment period.1 Two pathologists independently read the liver biopsies for each patient; a third pathologist performed adjudication if consensus could not be reached between the two pathologists.1
ESSENCE: A phase 3 efficacy and safety trial of Wegovy® injection in patients with MASH with liver fibrosis1,19
Primary end point results at week 721
With Wegovy®, significantly more patients achieved resolution of steatohepatitis and no worsening of liver fibrosis vs placebo1‖**††
Difference in response rate: 29 (95% CI: 21, 36)
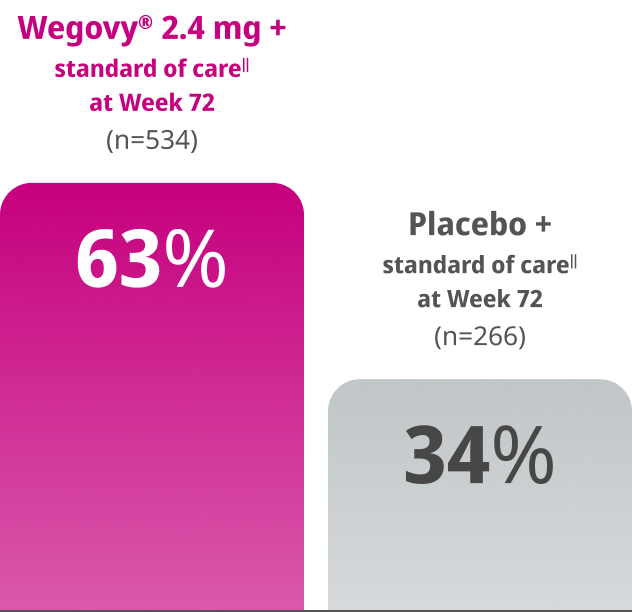
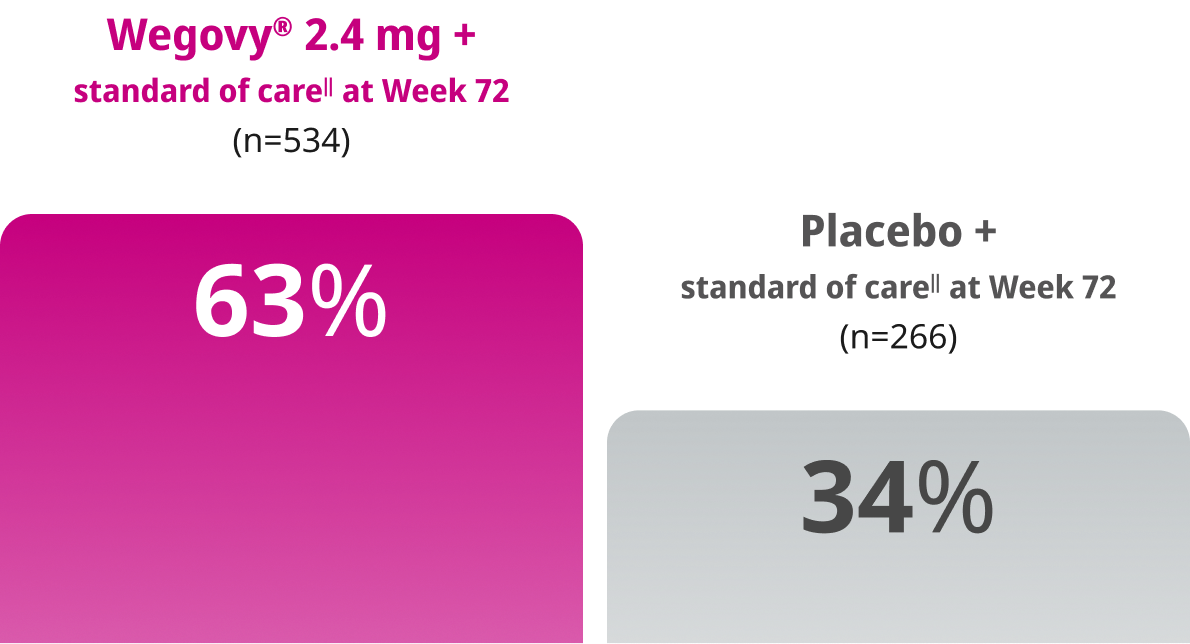
End point definition
- Elimination of hepatocyte ballooning
- No or mild lobular inflammation
- Any value for steatosis
- No worsening of liver fibrosis
Results were statistically significant
End point definition
- Elimination of hepatocyte ballooning
- No or mild lobular inflammation
- Any value for steatosis
- No worsening of liver fibrosis
Results were statistically significant
With Wegovy®, significantly more patients achieved improvement of liver fibrosis and no worsening of steatohepatitis vs placebo1‖**††
Difference in response rate: 14 (95% CI: 8, 21)
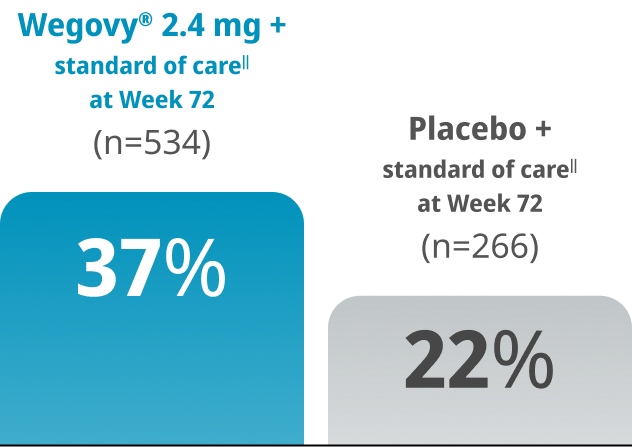
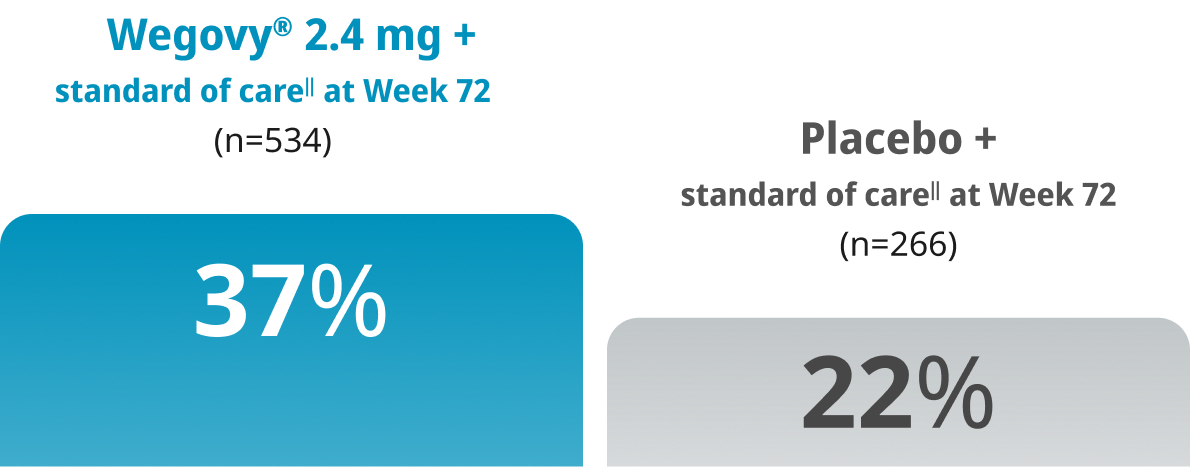
End point definition
- Improvement in liver fibrosis
by ≥1 stage
- No increase from baseline in ballooning, lobular inflammation, or steatosis
Results were statistically significant
End point definition
- Improvement in liver fibrosis
by ≥1 stage
- No increase from baseline in ballooning, lobular inflammation, or steatosis
Results were statistically significant
‖Investigators were encouraged to optimize treatment for type 2 diabetes, dyslipidemia, and cardiovascular risk management according to a standard of care guidance document.20
**End points were evaluated according to the MASH Clinical Research Network (CRN). Resolution of steatohepatitis is defined as a score of 0 to 1 for lobular inflammation, 0 for ballooning, and any value for steatosis. No worsening of steatohepatitis is defined as no increase from baseline in score for ballooning, lobular inflammation, or steatosis.1
††Estimated using pooled Mantel-Haenszel (MH) estimates stratified by baseline type 2 diabetes status (presence or absence) and baseline fibrosis stage (F2 or F3) with missing data handled by reference-based multiple imputation and 95% CIs calculated using Rubin’s rule to pool Sato’s estimate of standard errors across the imputed datasets.1
CI, confidence interval; NAS, nonalcoholic fatty liver disease (NAFLD) activity score.
Wegovy® pen is the first and only GLP-1 RA indicated for the treatment of noncirrhotic MASH with F2 to F3 fibrosis.1
Wegovy® for MASH: key access and coverage considerations
Wegovy® pen is the first-and-only GLP-1 RA approved for the treatment of noncirrhotic MASH with moderate to advanced liver fibrosis (consistent with stages F2 to F3 fibrosis), in combination with reduced-calorie diet and increased physical activity1
Coverage and out-of-pocket costs for Wegovy® for the MASH indication vary by health plan; patients should check with their individual health plan for details
Coverage for patients with public insurance (eg, Medicare and Medicaid) varies based on program and plan-specific policies for the MASH indication
A self-pay option is also available for eligible patients without insurance coverage
Explore coverage options and support programs
for Wegovy®
Disclaimer: Coverage, eligibility, and out-of-pocket costs vary by plan; patients should check with their health plan for details.
Support materials and coverage information for your organization
References: 1. Wegovy® [package insert]. Plainsboro, NJ: Novo Nordisk Inc. 2. Younossi ZM, Razavi H, Sherman M, et al. Addressing the high and rising global burden of metabolic dysfunction-associated steatotic liver disease (MASLD) and metabolic dysfunction-associated steatohepatitis (MASH): from the growing prevalence to payors' perspective. Aliment Pharmacol Ther. 2025;61(9):1467-1478. 3. Charlton M, Tonnu-Mihara I, Teng CC, et al. The clinical and economic burdens of metabolic dysfunction-associated steatohepatitis. J Med Econ. 2024;27(1):919-930. 4. Allen AM, Charlton M, Cusi K, et al. Guideline-based management of metabolic dysfunction-associated steatotic liver disease in the primary care setting. Postgrad Med. 2024;136(3):229-245. 5. Estes C, Anstee QM, Arias-Loste MT, et al. Modeling NAFLD disease burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the period 2016-2030. J Hepatol. 2018;69(4):896-904. 6. Cusi K, Isaacs S, Barb D, et al. American Association of Clinical Endocrinology clinical practice guideline for the diagnosis and management of nonalcoholic fatty liver disease in primary care and endocrinology clinical settings: co-sponsored by the American Association for the Study of Liver Diseases (AASLD). Endocr Pract. 2022;28(5):528-562. 7. Quek J, Chan KE, Wong ZY, et al. Global prevalence of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in the overweight and obese population: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2023;8(1):20-30. 8. Younossi ZM, Golabi P, de Avila L, et al. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: a systematic review and meta-analysis. J Hepatol. 2019;71(4):793-801. 9. Younossi ZM, Paik JM, Lazarus JV, et al. Projected global clinical, humanistic, and economic impact of metabolic dysfunction-associated steatohepatitis (MASH): the cost of inaction based on data from nine countries. Clin Gastroenterol Hepatol. 2025. S1542-3565(25)00757-8. 10. Rinella M, Cryer DR, Articolo A, Fisher T, Schneider J, Nadolsky K. Nonalcoholic steatohepatitis medical patient journey from the perspective of hepatologists, gastroenterologists and patients: a cross-sectional survey. BMC Gastroenterol. 2022;22(1):335. 11. Ortner N and Holzer H. 2025 U.S. organ and tissue transplants: estimated costs and utilization, emerging issues, and solutions. Milliman Report. Published February 13, 2025. Accessed March 5, 2026. https://www.milliman.com/en/insight/2025-us-organ-and-tissue-transplants-costs-utilization 12. Gordon SC, Kachru N, Parker E, Korrer S, Ozbay AB, Wong RJ. Health care use and costs among patients with nonalcoholic steatohepatitis with advanced fibrosis using the fibrosis-4 score. Hepatol Commun. 2020;4(7):998-1011. 13. Tapper EB, Bonafede M, Fishman J, et al. Healthcare resource utilization and costs of care in the United States for patients with non-alcoholic steatohepatitis. J Med Econ. 2023;26(1):348-356. 14. Rinella ME, Neuschwander-Tetri BA, Siddiqui MS, et al. AASLD practice guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology. 2023;77(5):1797-1835. 15. Cusi K, Abdelmalek MF, Apovian CM, et al. Metabolic dysfunction-associated steatotic liver disease (MASLD) in people with diabetes: the need for screening and early intervention. A consensus report of the American Diabetes Association. Diabetes Care. 2025;48(7):1057-1082. 16. Wattacheril JJ, Abdelmalek MF, Lim JK, Sanyal AJ. AGA clinical practice update on the role of noninvasive biomarkers in the evaluation and management of nonalcoholic fatty liver disease: expert review. Gastroenterology. 2023;165(4):1080-1088. 17. Godoy-Matos AF, Silva Júnior WS, Valerio CM. NAFLD as a continuum: from obesity to metabolic syndrome and diabetes. Diabetol Metab Syndr. 2020;12:60. 18. Eskridge W, Cryer DR, Schattenberg JM, et al. Metabolic dysfunction-associated steatotic liver disease and metabolic dysfunction-associated steatohepatitis: the patient and physician perspective. J Clin Med. 2023;12(19):6216. 19. Sanyal AJ, Newsome PN, Kliers I, et al. Phase 3 trial of semaglutide in metabolic dysfunction-associated steatohepatitis. N Engl J Med. 2025;392(21):2089-2099. 20. Newsome PN, Sanyal AJ, Engebretsen KA, et al. Semaglutide 2.4 mg in participants with metabolic dysfunction-associated steatohepatitis: baseline characteristics and design of the phase 3 ESSENCE trial. Aliment Pharmacol Ther. 2024;60(11-12):1525-1533.
Important Safety Information
WARNING: RISK OF THYROID C-CELL TUMORS
- In rodents, semaglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures. It is unknown whether Wegovy® causes thyroid C-cell tumors, including medullary thyroid carcinoma (MTC), in humans as human relevance of semaglutide-induced rodent thyroid C-cell tumors has not been determined
- Wegovy® is contraindicated in patients with a personal or family history of MTC or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). Counsel patients regarding the potential risk for MTC with the use of Wegovy® and inform them of symptoms of thyroid tumors (e.g. a mass in the neck, dysphagia, dyspnea, persistent hoarseness). Routine monitoring of serum calcitonin or using thyroid ultrasound is of uncertain value for early detection of MTC in patients treated with Wegovy®
Contraindications
- Wegovy® is contraindicated in patients with a personal or family history of MTC or in patients with MEN 2, and in patients with a prior serious hypersensitivity reaction to semaglutide or to any of the excipients in Wegovy®. Serious hypersensitivity reactions, including anaphylaxis and angioedema have been reported with Wegovy®
Warnings and Precautions
- Risk of Thyroid C-Cell Tumors: Patients should be further evaluated if serum calcitonin is measured and found to be elevated or thyroid nodules are noted on physical examination or neck imaging
- Acute Pancreatitis: Acute pancreatitis, including fatal and non-fatal hemorrhagic or necrotizing pancreatitis, has been observed in patients treated with GLP-1 receptor agonists, including Wegovy®. Observe patients carefully for signs and symptoms of acute pancreatitis, which may include persistent severe abdominal pain (sometimes radiating to the back), and which may or may not be accompanied by nausea or vomiting. If acute pancreatitis is suspected, discontinue Wegovy® and initiate appropriate management
- Acute Gallbladder Disease: Treatment with Wegovy® is associated with an increased occurrence of cholelithiasis and cholecystitis. The incidence of cholelithiasis and cholecystitis was higher in Wegovy® injection-treated pediatric patients aged ≥12 years than in injection-treated Wegovy® adults. In clinical trials in adult patients for weight reduction, cholelithiasis was reported by 1.6% of Wegovy® injection-treated patients and 0.7% of placebo patients. Cholecystitis was reported by 0.6% of Wegovy® injection-treated patients and 0.2% of placebo patients. In a clinical trial in pediatric patients aged ≥12 years, cholelithiasis was reported by 3.8% of Wegovy® injection-treated patients and 0% placebo treated patients. Cholecystitis was reported by 0.8% of Wegovy® injection-treated pediatric patients and 0% placebo treated patients. Substantial or rapid weight loss can increase the risk of cholelithiasis; however, the incidence of acute gallbladder disease was greater in Wegovy® patients than in placebo patients, even after accounting for the degree of weight loss. If cholelithiasis is suspected, gallbladder studies and appropriate clinical follow-up are indicated
- Hypoglycemia: Wegovy® lowers blood glucose and can cause hypoglycemia. In a trial of Wegovy® injection in adult patients with type 2 diabetes (T2D) and a BMI ≥27 kg/m2, hypoglycemia was reported in more patients treated with Wegovy® versus placebo. In glycemic control clinical trials, the risk of hypoglycemia was increased when semaglutide injection was used concomitantly with insulin or an insulin secretagogue (e.g., sulfonylurea). Patients with diabetes taking Wegovy® with an insulin or insulin secretagogue may have an increased risk of hypoglycemia, including severe hypoglycemia. The use of Wegovy® in patients with type 1 diabetes or in combination with insulin has not been evaluated. Inform patients of the risk of hypoglycemia and educate them on the signs and symptoms. Monitor blood glucose in patients with diabetes
- Acute Kidney Injury Due to Volume Depletion: There have been postmarketing reports of acute kidney injury, in some cases requiring hemodialysis, in patients treated with semaglutide. The majority of the reported events occurred in patients who experienced gastrointestinal reactions leading to dehydration such as nausea, vomiting, or diarrhea. Monitor renal function in patients reporting adverse reactions to Wegovy® that could lead to volume depletion, especially during initiation and escalation of Wegovy®
- Severe Gastrointestinal (GI) Adverse Reactions: Use of Wegovy® has been associated with GI adverse reactions, sometimes severe. In adult clinical trials, severe GI adverse reactions were reported more frequently among patients receiving Wegovy® injection (4.1%) than placebo (0.9%). Severe GI adverse reactions have also been reported postmarketing with GLP-1 receptor agonists. Wegovy® is not recommended in patients with severe gastroparesis
- Hypersensitivity Reactions: Serious hypersensitivity reactions (e.g., anaphylaxis, angioedema) have been reported with Wegovy®. If hypersensitivity reactions occur, discontinue use of Wegovy®, treat promptly per standard of care, and monitor until signs and symptoms resolve. Use caution in a patient with a history of anaphylaxis or angioedema with another GLP-1 receptor agonist
- Diabetic Retinopathy Complications in Patients with T2D: In a trial of adult patients with T2D and BMI ≥27 kg/m2, diabetic retinopathy was reported by 4% of Wegovy® injection-treated patients and 2.7% of placebo patients. Rapid improvement in glucose control has been associated with a temporary worsening of diabetic retinopathy. Patients with a history of diabetic retinopathy should be monitored for progression of diabetic retinopathy
- Heart Rate Increase: Mean increases in resting heart rate of 1 to 4 beats per minute (bpm) were observed in Wegovy® injection-treated adult patients compared to placebo in clinical trials. More adults treated with Wegovy® injection compared with placebo had maximum changes from baseline of 10 to 19 bpm (41% vs 34%) and 20 bpm or more (26% vs 16%). In a clinical trial in pediatric patients aged ≥12 years with normal baseline heart rate, more patients treated with Wegovy® injection compared to placebo had maximum changes in heart rate of 20 bpm or more (54% vs 39%). Monitor heart rate at regular intervals and instruct patients to report palpitations or feelings of a racing heartbeat while at rest. If patients experience a sustained increase in resting heart rate, discontinue Wegovy®
- Pulmonary Aspiration During General Anesthesia or Deep Sedation: Wegovy® delays gastric emptying. There have been rare postmarketing reports of pulmonary aspiration in patients receiving GLP-1 receptor agonists undergoing elective surgeries or procedures requiring general anesthesia or deep sedation who had residual gastric contents despite reported adherence to preoperative fasting recommendations. Instruct patients to inform healthcare providers prior to any planned surgeries or procedures if they are taking Wegovy®
Adverse Reactions
- Most common adverse reactions (incidence ≥5%) are: nausea, diarrhea, vomiting, constipation, abdominal pain, dysesthesia, headache, fatigue, dyspepsia, dizziness, abdominal distention, eructation, hypoglycemia in patients with T2D, flatulence, gastroenteritis, gastroesophageal reflux disease, and hair loss
Drug Interactions
- When initiating Wegovy®, consider reducing the dose of concomitantly administered insulin secretagogues or insulin to reduce the risk of hypoglycemia. The addition of Wegovy® in patients treated with insulin has not been evaluated
- Wegovy® causes a delay of gastric emptying and has the potential to impact the absorption of concomitantly administered oral medications. Monitor the effects of oral medications concomitantly administered with Wegovy®. Consider increased clinical or laboratory monitoring for medications that have a narrow therapeutic index or that require clinical monitoring
Use in Specific Populations
- Pregnancy: May cause fetal harm. When pregnancy is recognized, discontinue Wegovy®. Discontinue Wegovy® in patients at least 2 months before a planned pregnancy
- Pediatric: Adverse reactions with Wegovy® in pediatric patients aged ≥12 years with obesity were similar to those reported in adults in weight reduction trials. Pediatric patients ≥12 years treated with Wegovy® injection had greater incidences of cholelithiasis, cholecystitis, hypotension, rash, and urticaria compared to adults treated with Wegovy®. There are insufficient data in pediatric patients with T2D treated with Wegovy® for obesity to determine if there is an increased risk of hypoglycemia with Wegovy® injection treatment similar to that reported in adults
The safety and effectiveness of Wegovy® injection have not been established in pediatric patients to reduce the risk of major adverse CV events, to reduce excess body weight and maintain weight reduction long term in those <12 years, or for the treatment of noncirrhotic MASH - Geriatric: In the CV outcomes trial, patients ≥75 years reported more hip and pelvis fractures on Wegovy® injection than placebo. Patients aged ≥75 years (Wegovy® injection and placebo) reported more serious adverse reactions overall compared to younger adult patients
- Type 2 Diabetes: Administration of Wegovy® injection resulted in less weight reduction in patients with T2D and obesity or overweight compared to those without T2D and obesity or overweight
Please click here for Wegovy® Prescribing Information, including Boxed Warning.
Indications and Usage
Wegovy® (semaglutide) injection 2.4 mg is indicated in combination with a reduced calorie diet and increased physical activity:
- for the treatment of noncirrhotic metabolic dysfunction-associated steatohepatitis (MASH), formerly known as nonalcoholic steatohepatitis (NASH), with moderate to advanced liver fibrosis (consistent with stages F2 to F3 fibrosis) in adults. The indication for MASH is approved under accelerated approval based on improvement of MASH and fibrosis. Continued approval for this indication may be contingent upon the verification and description of clinical benefit in a confirmatory trial.
- to reduce the risk of major adverse cardiovascular (CV) events (CV death, non-fatal myocardial infarction, or non-fatal stroke) in adults with established CV disease and either obesity or overweight
- to reduce excess body weight and maintain weight reduction long term in adults and pediatric patients aged 12 years and older with obesity and adults with overweight in the presence of at least one weight-related comorbid condition
Limitations of Use:
Concomitant use of Wegovy® injection with other semaglutide-containing products or with any GLP-1 receptor agonist is not recommended
Important Safety Information for Wegovy®
WARNING: RISK OF THYROID C-CELL TUMORS
- In rodents, semaglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures. It is unknown whether Wegovy® causes thyroid C-cell tumors, including medullary thyroid carcinoma (MTC), in humans as human relevance of semaglutide-induced rodent thyroid C-cell tumors has not been determined
- Wegovy® is contraindicated in patients with a personal or family history of MTC or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). Counsel patients regarding the potential risk for MTC with the use of Wegovy® and inform them of symptoms of thyroid tumors (e.g. a mass in the neck, dysphagia, dyspnea, persistent hoarseness). Routine monitoring of serum calcitonin or using thyroid ultrasound is of uncertain value for early detection of MTC in patients treated with Wegovy®
Contraindications
- Wegovy® is contraindicated in patients with a personal or family history of MTC or in patients with MEN 2, and in patients with a prior serious hypersensitivity reaction to semaglutide or to any of the excipients in Wegovy®. Serious hypersensitivity reactions, including anaphylaxis and angioedema have been reported with Wegovy®
Important Safety Information
WARNING: RISK OF THYROID C-CELL TUMORS
- In rodents, semaglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures. It is unknown whether Wegovy® causes thyroid C-cell tumors, including medullary thyroid carcinoma (MTC), in humans as human relevance of semaglutide-induced rodent thyroid C-cell tumors has not been determined
- Wegovy® is contraindicated in patients with a personal or family history of MTC or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). Counsel patients regarding the potential risk for MTC with the use of Wegovy® and inform them of symptoms of thyroid tumors (e.g. a mass in the neck, dysphagia, dyspnea, persistent hoarseness). Routine monitoring of serum calcitonin or using thyroid ultrasound is of uncertain value for early detection of MTC in patients treated with Wegovy®
Contraindications
- Wegovy® is contraindicated in patients with a personal or family history of MTC or in patients with MEN 2, and in patients with a prior serious hypersensitivity reaction to semaglutide or to any of the excipients in Wegovy®. Serious hypersensitivity reactions, including anaphylaxis and angioedema have been reported with Wegovy®
Warnings and Precautions
- Risk of Thyroid C-Cell Tumors: Patients should be further evaluated if serum calcitonin is measured and found to be elevated or thyroid nodules are noted on physical examination or neck imaging
- Acute Pancreatitis: Acute pancreatitis, including fatal and non-fatal hemorrhagic or necrotizing pancreatitis, has been observed in patients treated with GLP-1 receptor agonists, including Wegovy®. Observe patients carefully for signs and symptoms of acute pancreatitis, which may include persistent severe abdominal pain (sometimes radiating to the back), and which may or may not be accompanied by nausea or vomiting. If acute pancreatitis is suspected, discontinue Wegovy® and initiate appropriate management
- Acute Gallbladder Disease: Treatment with Wegovy® is associated with an increased occurrence of cholelithiasis and cholecystitis. The incidence of cholelithiasis and cholecystitis was higher in Wegovy® injection-treated pediatric patients aged ≥12 years than in injection-treated Wegovy® adults. In clinical trials in adult patients for weight reduction, cholelithiasis was reported by 1.6% of Wegovy® injection-treated patients and 0.7% of placebo patients. Cholecystitis was reported by 0.6% of Wegovy® injection-treated patients and 0.2% of placebo patients. In a clinical trial in pediatric patients aged ≥12 years, cholelithiasis was reported by 3.8% of Wegovy® injection-treated patients and 0% placebo treated patients. Cholecystitis was reported by 0.8% of Wegovy® injection-treated pediatric patients and 0% placebo treated patients. Substantial or rapid weight loss can increase the risk of cholelithiasis; however, the incidence of acute gallbladder disease was greater in Wegovy® patients than in placebo patients, even after accounting for the degree of weight loss. If cholelithiasis is suspected, gallbladder studies and appropriate clinical follow-up are indicated
- Hypoglycemia: Wegovy® lowers blood glucose and can cause hypoglycemia. In a trial of Wegovy® injection in adult patients with type 2 diabetes (T2D) and a BMI ≥27 kg/m2, hypoglycemia was reported in more patients treated with Wegovy® versus placebo. In glycemic control clinical trials, the risk of hypoglycemia was increased when semaglutide injection was used concomitantly with insulin or an insulin secretagogue (e.g., sulfonylurea). Patients with diabetes taking Wegovy® with an insulin or insulin secretagogue may have an increased risk of hypoglycemia, including severe hypoglycemia. The use of Wegovy® in patients with type 1 diabetes or in combination with insulin has not been evaluated. Inform patients of the risk of hypoglycemia and educate them on the signs and symptoms. Monitor blood glucose in patients with diabetes
- Acute Kidney Injury Due to Volume Depletion: There have been postmarketing reports of acute kidney injury, in some cases requiring hemodialysis, in patients treated with semaglutide. The majority of the reported events occurred in patients who experienced gastrointestinal reactions leading to dehydration such as nausea, vomiting, or diarrhea. Monitor renal function in patients reporting adverse reactions to Wegovy® that could lead to volume depletion, especially during initiation and escalation of Wegovy®
- Severe Gastrointestinal (GI) Adverse Reactions: Use of Wegovy® has been associated with GI adverse reactions, sometimes severe. In adult clinical trials, severe GI adverse reactions were reported more frequently among patients receiving Wegovy® injection (4.1%) than placebo (0.9%). Severe GI adverse reactions have also been reported postmarketing with GLP-1 receptor agonists. Wegovy® is not recommended in patients with severe gastroparesis
- Hypersensitivity Reactions: Serious hypersensitivity reactions (e.g., anaphylaxis, angioedema) have been reported with Wegovy®. If hypersensitivity reactions occur, discontinue use of Wegovy®, treat promptly per standard of care, and monitor until signs and symptoms resolve. Use caution in a patient with a history of anaphylaxis or angioedema with another GLP-1 receptor agonist
- Diabetic Retinopathy Complications in Patients with T2D: In a trial of adult patients with T2D and BMI ≥27 kg/m2, diabetic retinopathy was reported by 4% of Wegovy® injection-treated patients and 2.7% of placebo patients. Rapid improvement in glucose control has been associated with a temporary worsening of diabetic retinopathy. Patients with a history of diabetic retinopathy should be monitored for progression of diabetic retinopathy
- Heart Rate Increase: Mean increases in resting heart rate of 1 to 4 beats per minute (bpm) were observed in Wegovy® injection-treated adult patients compared to placebo in clinical trials. More adults treated with Wegovy® injection compared with placebo had maximum changes from baseline of 10 to 19 bpm (41% vs 34%) and 20 bpm or more (26% vs 16%). In a clinical trial in pediatric patients aged ≥12 years with normal baseline heart rate, more patients treated with Wegovy® injection compared to placebo had maximum changes in heart rate of 20 bpm or more (54% vs 39%). Monitor heart rate at regular intervals and instruct patients to report palpitations or feelings of a racing heartbeat while at rest. If patients experience a sustained increase in resting heart rate, discontinue Wegovy®
- Pulmonary Aspiration During General Anesthesia or Deep Sedation: Wegovy® delays gastric emptying. There have been rare postmarketing reports of pulmonary aspiration in patients receiving GLP-1 receptor agonists undergoing elective surgeries or procedures requiring general anesthesia or deep sedation who had residual gastric contents despite reported adherence to preoperative fasting recommendations. Instruct patients to inform healthcare providers prior to any planned surgeries or procedures if they are taking Wegovy®
Adverse Reactions
- Most common adverse reactions (incidence ≥5%) are: nausea, diarrhea, vomiting, constipation, abdominal pain, dysesthesia, headache, fatigue, dyspepsia, dizziness, abdominal distention, eructation, hypoglycemia in patients with T2D, flatulence, gastroenteritis, gastroesophageal reflux disease, and hair loss
Drug Interactions
- When initiating Wegovy®, consider reducing the dose of concomitantly administered insulin secretagogues or insulin to reduce the risk of hypoglycemia. The addition of Wegovy® in patients treated with insulin has not been evaluated
- Wegovy® causes a delay of gastric emptying and has the potential to impact the absorption of concomitantly administered oral medications. Monitor the effects of oral medications concomitantly administered with Wegovy®. Consider increased clinical or laboratory monitoring for medications that have a narrow therapeutic index or that require clinical monitoring
Use in Specific Populations
- Pregnancy: May cause fetal harm. When pregnancy is recognized, discontinue Wegovy®. Discontinue Wegovy® in patients at least 2 months before a planned pregnancy
- Pediatric: Adverse reactions with Wegovy® in pediatric patients aged ≥12 years with obesity were similar to those reported in adults in weight reduction trials. Pediatric patients ≥12 years treated with Wegovy® injection had greater incidences of cholelithiasis, cholecystitis, hypotension, rash, and urticaria compared to adults treated with Wegovy®. There are insufficient data in pediatric patients with T2D treated with Wegovy® for obesity to determine if there is an increased risk of hypoglycemia with Wegovy® injection treatment similar to that reported in adults
The safety and effectiveness of Wegovy® injection have not been established in pediatric patients to reduce the risk of major adverse CV events, to reduce excess body weight and maintain weight reduction long term in those <12 years, or for the treatment of noncirrhotic MASH - Geriatric: In the CV outcomes trial, patients ≥75 years reported more hip and pelvis fractures on Wegovy® injection than placebo. Patients aged ≥75 years (Wegovy® injection and placebo) reported more serious adverse reactions overall compared to younger adult patients
- Type 2 Diabetes: Administration of Wegovy® injection resulted in less weight reduction in patients with T2D and obesity or overweight compared to those without T2D and obesity or overweight
Please click here for Wegovy® Prescribing Information, including Boxed Warning.
Indications and Usage
Wegovy® (semaglutide) injection 2.4 mg is indicated in combination with a reduced calorie diet and increased physical activity:
- for the treatment of noncirrhotic metabolic dysfunction-associated steatohepatitis (MASH), formerly known as nonalcoholic steatohepatitis (NASH), with moderate to advanced liver fibrosis (consistent with stages F2 to F3 fibrosis) in adults. The indication for MASH is approved under accelerated approval based on improvement of MASH and fibrosis. Continued approval for this indication may be contingent upon the verification and description of clinical benefit in a confirmatory trial.
- to reduce the risk of major adverse cardiovascular (CV) events (CV death, non-fatal myocardial infarction, or non-fatal stroke) in adults with established CV disease and either obesity or overweight
- to reduce excess body weight and maintain weight reduction long term in adults and pediatric patients aged 12 years and older with obesity and adults with overweight in the presence of at least one weight-related comorbid condition
Limitations of Use:
Concomitant use of Wegovy® injection with other semaglutide-containing products or with any GLP-1 receptor agonist is not recommended