Information and services for you, education and support for your patients—across all of our therapy areas.
Diabetes
Diabetes
Actor portrayal
Obesity
Obesity
Actor portrayal
Rare Bleeding
Disorders
Rare Bleeding
Disorders
Actor portrayal
Growth-Related
Disorders
Growth-Related
Disorders
Actor portrayal
Rare Renal
Disorders
Rare Renal
Disorders
Actor portrayal
How can we help you today?
Information about Hormone Replacement Therapy due to menopause
Featured in diabetes

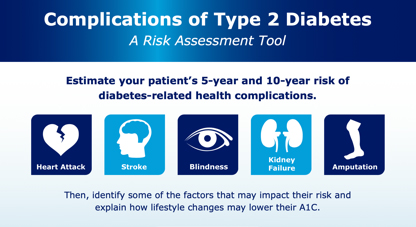
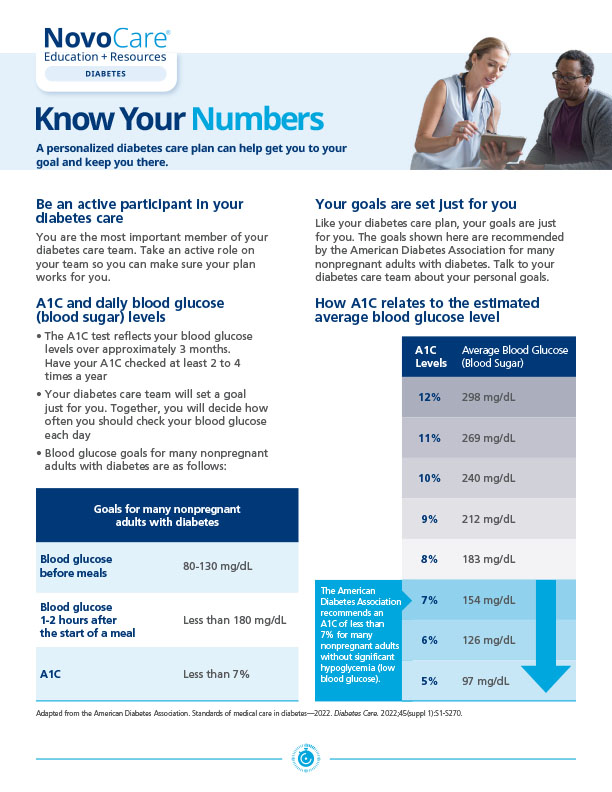
Patient educational materials on diabetes

Featured in obesity
Obesity is a disease
Explore the science behind obesity, why your patients with obesity struggle to lose weight and how you can make a difference.
Upcoming obesity conferences
Connect with organizations that provide in-depth obesity information and educational opportunities.


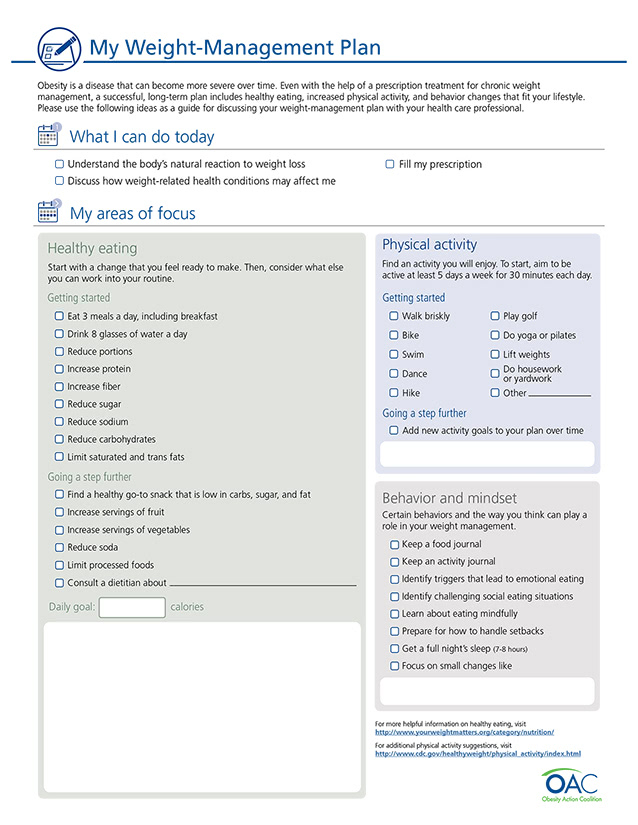
Obesity education materials for your patients
Share these disease education resources with patients at all stages of their weight-loss journey.

Join for access to sample ordering, device training, educational materials, product information, personalized resource updates, and more
Actor portrayal

Join for access to sample ordering, device training, educational materials, product information, personalized resource updates, and more
Actor portrayal
Featured in rare bleeding disorders

Patient educational materials on rare bleeding disorders
Understanding acquired hemophilia
Acquired hemophilia appears spontaneously in people who were not born with hemophilia. Learn the signs of this rare condition.
Actor portrayal
Featured in growth-related disorders

Defining pediatric growth-related disorders
Learn the basics of pathological conditions that are associated with short stature in children, including growth hormone deficiency, genetic syndromes, and other growth-related disorders.
Actor portrayal
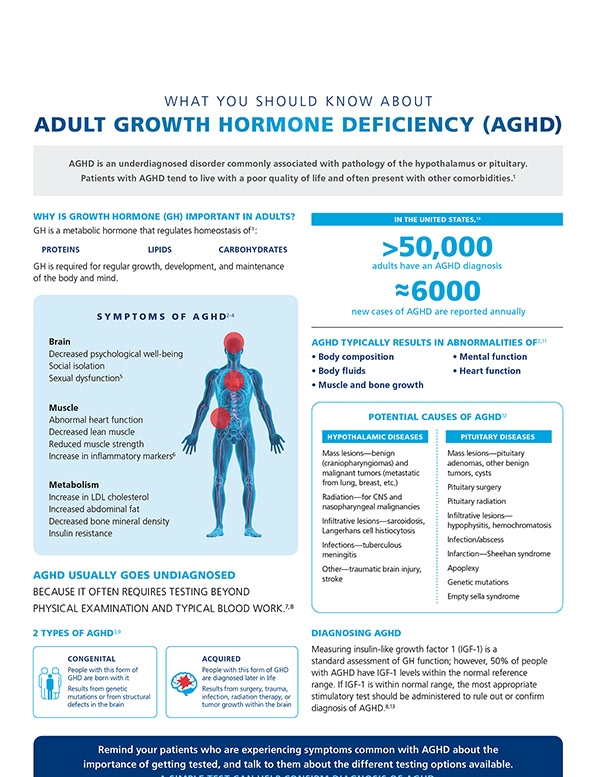
Overview on adult growth hormone deficiency
Actor portrayal
Affordability resources for your patients
NovoCare® provides affordability and access support resources to help your eligible patients obtain the medicine that’s right for them.
Actor portrayal